Update: 24 April 2024
Depression, Suicide, Violence
Article contributors: R. Malter, Dr. David L. Watts, J. Casper, C. Ac.
Advances in understanding the biochemical markers associated with psychological dysfunction have far-reaching implications for safe, effective therapeutic solutions. hTMA data can help an experienced clinician develop protocols for the treatment and prevention of addiction, aggression, anxiety, bipolar disorder, depression, suicide and other psychological conditions.
Contents
- Emotions
- Responding to Environmental Stressors in a Toxic Environment
- hTMA Screening for Emotional Health
- Traumatic Memory
- Suicide
- Suicide - the Ultimate Escape
- Suicide Prevention
- Tragedy and Mental Health
- Rage and Outrage
- Copper Toxicity, and Sodium/Potassium Ratios in Psychological Functioning
- Psychiatric drug-induced Chronic Brain Impairment (CBI)
- Copper and Psychology
- Personality Characteristics Reflected in hTMA Patterns
- Aggressive Behavior
- Anxiety
- Addiction
- Mania and Depression (Bipolar)
- Depression
- Conclusion
- Resources
- References
Emotions
J. Casper, C. Ac.

Our emotions are what allow us to fully experience life. In fact, our highly sophisticated emotional response system is probably the most important reason why we have evolved as the dominant species on this planet.
Biologically, emotions are a primary aspect of the autonomic stress-response system. Yet emotional sensitivity and expression varies tremendously between individuals. This can be more easily understood by looking at the biology of a single cell. A single cell observed in a petri dish responds to its environment in one of two ways. If a toxin is introduced to its environment, it withdraws as a protective response, when a nutrient is introduced, it moves forward in a growth response. This mutually exclusive "protection" or "growth" cellular motional response is the foundation of a highly complex emotion response system in multi-cellular organisms (like human beings).
Emotional reactions are the result of the extensive interactions between the nervous system and the endocrine system (neuroendocrinology), including the biological features of the cells and how they communicate. The nervous and endocrine systems act together to regulate the psychophysiological processes of the human body. This means that emotions are fundamentally biochemical in nature. And biochemical imbalances can reek havoc on emotions. The ability to adequately respond to environmental stressors is reliant on available cellular energy, and how well one can recover from the stressful event.
Responding to Environmental Stressors in a Toxic Environment
Recently, a story about an international mercury-emissions treaty was covered in the media. More than 140 countries are working to adopt a legally binding agreement to reduce mercury emissions. A signing ceremony will be held later this year, nations then must begin formally ratifying the treaty before it comes into force several years from now. Joe DiGangi, a science adviser with the environmental advocacy group IPEN, commented that while the treaty is "a first step," it is not tough enough to achieve its aim of reducing overall emissions. Or, too little, too late. Once put into the environment, these heavy metals do not go away or break down, they just keep moving around.
This problem is not new. Scientists have known about the hazards of mercury (along with many other toxic elements such as lead, arsenic, cadmium, aluminum and more) for many decades. In the early 1970's Henry A. Schroeder, M.D. published two books which informed the public on the current research about this issue, "The Trace Elements and Man" and "Pollution, Profits and Progress." At the same time, Carl C. Pfeiffer, Ph. D., M. D. wrote "Mental and Elemental Nutrients," which explained the research behind the physical and emotional effects of these toxic elements and of the effects of nutrient mineral imbalances on our psychology. The element lead alone could be responsible for the increases in hyperactivity in our children. Combine lead with mercury, aluminum and cadmium and you have a deadly cocktail for mental imbalances and brain dysfunction and deterioration.
Important public health information is frequently suppressed. In an article by Sheila Kaplan from Harvard University's Edmund J. Safra Center for Ethics titled, "White House Stalls EPA Report" she explains how a Environmental Protection Agency (EPA) report concluded that children exposed to toxic chemicals develop learning disabilities, asthma and other major health problems. This report has been sidetracked indefinitely amid fierce opposition from the $674 billion chemical industry. On Thursday, December 27, EPA chief Lisa Jackson, who was praised by environmentalists but vilified by industry and many congressional lawmakers, said she would resign in January.
Just look at us. Everything is backwards; everything is upside down. Doctors destroy health. Lawyers destroy justice. Universities destroy knowledge. Governments destroy freedom. The major media destroy information. And religions destroy spirituality. Michael Ellner
The unsurprising response of the medical industry has been to suppress this important information about the psychological effects of toxins, and instead promote "treatment" of the resulting mental disorders. Treatment with toxic drugs that actually result in further psychophysiological imbalances. All of these so called "new" psychological disorders are simply rearranged groups of symptoms (symptom clusters) conveniently organized to be coupled with a targeted pharmaceutical "remedy." In fact, the underlying reason for these wide-ranging symptomatic reactions has more to do with an individual's unique cellular mineral imbalances, and their corresponding inability to respond adequately to the given environmental stressor(s).
hTMA Screening for Emotional Health
hTMA screening provides clinicians with an accurate stress and energy profile which also measures nutrient mineral levels and ratios. Essential nutrient minerals are important in the regulation of glucose metabolism, autonomic neurological functions (sympathetic and parasympathetic), neuroendocrine activities (adrenal and thyroid glands) and immunological functions (humoral and cellular). It is well understood that depression is a low energy condition often related to diminished thyroid and/or adrenal activity. And because the adrenal glands are involved in the regulation of sodium and potassium they play a major role in the emotions that include anxiety, panic disorder, anger and rage. hTMA reveals biochemical and nutrient information which reflects psychophysiological status and has meaningful predictive and preventive value.
Having distorted mineral levels is like trying to look at the heavens through a cloudy telescope. You can never see the true picture. Only when an individual's minerals become balanced will he be able to see the world as it really is, instead of the way he wants to see it. Dr. Paul Eck
Traumatic Memory
Loss of a loved one, or any emotionally traumatic event for that matter, has significant impact on memory. Functionally, memory also is a biochemical process. The initial shock of a traumatic event will disrupt emotional stability (balanced biochemistry). How well, and how quickly one recovers emotional stability depends on their stress response ability. The pain of heartache is an emotion we all will experience in life. Healing emotional trauma is possible.
In healthy individuals, over time, intense sadness can result in emotional strengthening. Emotion contains the word motion. It is derived on the French model of movoir: motion, from esmovoir to set in motion, move the feelings. Traumatic emotion can motivate an individual into action which requires great strength of character and empathy. Nothing can be a substitute for love and interpersonal connections — the ultimate emotional healers.
When there is an impoverished stress response, traumatic memories can result in post-traumatic stress disorder (PTSD). The person's ability to move through the emotions becomes stuck, and the intense trauma is repeated, over and over, brought on by the slightest triggering event. This can lead to attempts to escape through drugs, reckless behavior or ultimately, suicide. The dramatically increasing rates of PTSD and suicide amongst our returning veterans is indicative of the increased toxic body burden and nutritional deficiencies in our youth today. When the stress response is strengthened through improved mineral balances and decreased toxicity, the PTSD sufferer can then move through the emotion in a healthy way, thus adding it to their life experience and being able to actually "move on."
Suicide
In polite society, suicide is a taboo topic. Why do we accept this? At age 75, my father unexpectedly committed a violent form of suicide. At age 21, shortly after having been diagnosed as "schizophrenic" and put on psychotropic drugs, my husband's childhood best friend used his father's shotgun to kill both his parents and his younger sister before he turned it on himself. The best man at our wedding committed suicide at 37. Due to back pain, he had become addicted to the Percocet® (acetaminophen and oxycodone) prescribed by his doctors. Sadly, I could continue. Suicide is personal for many of us. The time to begin a meaningful cultural dialog is long overdue.
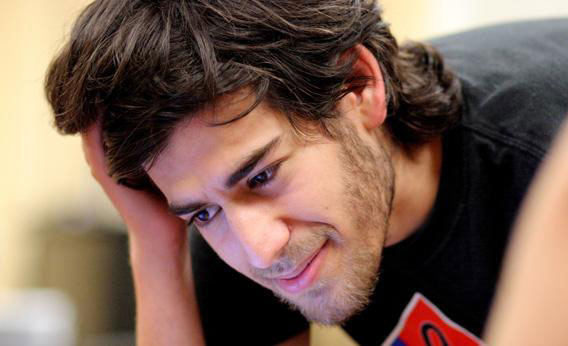
Aaron Swartz (1986 – 2013). Aaron was a beautiful, very bright light of hope and possibility. He showed us the need for change, and how to do it. His short life was proof of the power of ‘one for all.’ We are certain that his legacy will have a planet-wide ripple effect, inspiring all of us who love him to mobilize courage and collaborate for social justice.
Aaron's commitment to social justice was profound, and defined his life. He was instrumental to the defeat of an Internet censorship bill; he fought for a more democratic, open, and accountable political system; and he helped to create, build, and preserve a dizzying range of scholarly projects that extended the scope and accessibility of human knowledge. He used his prodigious skills as a programmer and technologist not to enrich himself but to make the Internet and the world a fairer, better place. His deeply humane writing touched minds and hearts across generations and continents. He earned the friendship of thousands and the respect and support of millions more. Statement from Arron's family and his partner, Taren Stinebricker-Kaufman
Our deepest hope is that the world-wide heartbreak felt at the tragic loss of visionary Aaron Swartz will motivate us to stop the insanity. That Aaron's powerful spirit will live on with all of us continuing his work to realize social evolution.
Psychiatric care might, at least in part, cause suicide. Taking psychiatric medications makes people nearly 6 times more likely to kill themselves, while having spent time in a psychiatric hospital (in the previous year) makes them over 44 times more likely to kill themselves. Social Psychiatry and Psychiatric Epidemiology
Suicide - the Ultimate Escape
The high-pressure, highly-complex culture we live in significantly diminishes our biochemical ability to respond to environmental stressors. Exhaustion drives many people to seek some form of emotional escape. And we have ways to escape. People may engage in a favorite activity like exercise or a hobby. Entertainment attracts a lot of us. We may turn to stimulants like coffee, alcohol, cigarettes, pharmaceutical or illicit drugs to feel better. Suicide is the last, and ultimate, form of escape. Suicide is a complete breakdown in one's ability to respond to stress.
Suicide Prevention
Suicide is absolutely preventable. Not unlike cancer, suicide is the final stop on a long journey that precedes it. And although we avoid thinking or talking about it, suicide often comes as no surprise. There are many stages of deteriorating biochemical imbalance that can be identified, and reversed, long before this devastating systems-wide stress response failure occurs. hTMA is the most effective mental health screen developed today, because it analyzes the biochemistry responsible for stress response as well as the presence of neurotoxic metals. Standard psychiatric mental health screens are designed to identify "symptom clusters" in order to match them with a pharmacological-based suppression therapy. Leading research shows that drug therapy designed to mask symptoms ultimately makes matters worse. Over time, mental health deteriorates. Health is not restored. When properly analyzed, hTMA data provides a clear profile of the patient's biochemistry. This information allows the knowledgable practitioner to recommend an individualized nutritional protocol to help rebalance mineral levels and ratios. Biochemical balance restores psychophysiological wellness and resilience.

The tragedies at Sandy Hook Elementary, Columbine, Aurora, Colorado, Virginia Tech (and others) were all preventable. The most formidable world super-power is not a government. Pharmaceutical drugs are the most profitable products in history. This is an industry that is fundamentally anti-life, and it targets our children. It's products toxic effluence is destroying the environment. The question is, are we willing to change the profitable mental health paradigm?
For the last 33 years, Dr. David Healy, an Irish psychiatrist and professor at Cardiff University School of Medicine in Wales, has written heavily researched university press books and academic journal articles on various aspects of psycho pharmaceuticals. Dr. Healy has tried to draw attention to the connection between the increasing use of antidepressants and antipsychotics and the increasing number of school shootings. On a Jan. 30, 2013 blog post and video on Rxisk.org, he claimed that 90 percent of school shooters in North America and Europe were on or withdrawing from psychopharmaceutical medications at the time of the incident. There is a list on SSIR Stories.com that documents perpetrators and the drugs they were on for violent acts committed in schools 1988-2011.
Back to TopTragedy and Mental Health
R. Malter
The tragic Sandy Hook Elementary event in Newtown, CT was an emotional roller coaster for us. It is a natural reaction to try to make some sense out of this horrific senseless mass murder. All of us are searching for answers. Could such a tragedy have been prevented?
Some media people and politicians say we need more "mental health" care. That is certainly an important issue, but it depends on what kind of "mental health" care you are considering. Helping people deal with their fears, anger, stresses, and conflicts can be very beneficial for large numbers of people. Providing them with proper nutritional supplements (guided by hTMA) can help reduce their stress and restore better emotional control. But, we don't think this is what proponents of more "mental health" services have in mind.
The dominant approach to "mental health" services today is a superficial psychiatric "diagnosis" and psychotropic drug "treatment." However, there is an irony in this situation. In the vast majority of cases of bizarre mass murders in the past few decades, the murderer was already on at least one or more toxic psychotropic drugs or they were withdrawing from these toxic drugs. Drugging people with an array of psychotropic drugs can damage brain function and make them more homicidal/suicidal. There is much evidence of the brain-damaging effects of medications.
To learn more about the role of psychotropic drugs in mass murder/suicide events, a great resource is Dr. Ann Blake Tracy, a Health Psychologist. She has been researching this subject for more than 20 years and has found a strong connection between various psychotropic drugs and homicidal/suicidal behavior. Her book Prozac: Panacea or Pandora thoroughly covers the dangers of these psychotropic drugs, especially bringing on violent behavior.
Dr. Peter Breggin, a psychiatrist, warns of the dangers of many of these psychotropic drugs. One of his books is Toxic Psychiatry. Perhaps not surprisingly, the media and politicians have avoided discussing the role of toxic psychotropic drugs in these horrific mass murder/suicide cases. Expanding "mental health" services dominated by the psychiatry/psychotropic drug industry makes no sense. Drs. Tracy and Breggin have already documented a strong relationship between these mind altering drugs and violent behavior. hTMA mineral balancing is a much safer, healthier alternative that can provide effective help to most people who need mental health services.
Is this what we really need? More diagnoses, more patients, more psychiatric drugs spreading like a chemical plague throughout the world? We are now learning that the longer-term use of some of these psychiatric drugs can cause chronic mental disability.
Several of my books (for example and for example), recently bolstered by Robert Whitaker's, leave no doubt that the evidence for longer-term efficacy (months or years) is insufficient, while the evidence for longer-term harm is escalating.
Studies are showing that this chronicity actually reflects physical damage to the brain. Studies revealing changes to the brain from antidepressants, from the so-called antipsychotic drugs (the neuroleptics), from stimulants and from benzodiazepines and prescription sleep medications -- are piling up, documenting patient risks.
In my professional experience, psychiatric drug-induced chronic brain impairment is now a much greater threat to society than the emotional problems that the drugs are supposed to treat.
Peter R. Breggin, M.D.
Rage and Outrage
The distinction between rage and outrage is important to understand.
- Rage.
- Some people can become so overtaken with intense emotion, they "shake and tremble with rage." They feel as if they could lose control of themselves at any moment. And worry that if that were to happen, they feel as if they would explode and could actually kill someone. Another experience is being so emotionally out of control that they think they might "go crazy" and be committed to a psychiatric hospital. With both experiences, there is an intense amount of anxiety that only adds to the sense of being emotionally out of control.
- Outrage.
- Another intense emotion is the feeling of outrage directed toward some person(s) who have done something that is overtly hurtful to another. The feeling of outrage is a natural human response to an outrageous event or action. When a person feels outrage, it is usually experienced as a distinctly different feeling from the feeling of rage, although both emotions are accompanied by anxiety. With rage and anxiety, the reaction is usually so intense that the person's body cannot contain the emotional intensity. This may lead to a shaking and trembling feeling and the apprehension of losing emotional control. Where with outrage, there also is intense emotion, but there is a fearless attitude. Fearlessness is a very different emotion from anxiety or panic.
Rage, accompanied by intense anxiety, is related to the inner child who carries feelings of anxiety and terror, but also anger and rage towards insensitive, punitive, abusing adults. Rage is ultimately an impotent child-like feeling with no way to express it safely. The intensity of the stress response associated with rage and anxiety also inflates judgmental messages such as "you shouldn't be this angry; you have no right to such angry feelings; something terrible will happen to you if you can't control yourself; if you are so emotional, you must be crazy." The rage, fear and anxiety become so intense that the child's body cannot contain the feelings; they overflow and elicit physical shaking and trembling reactions.
Outrage is associated with a mature, resilient, warrior archetype. It evokes strong maternal and paternal instincts, and is a powerful, fearless disposition. Psychologically, outrage it is a very different experience than the impotent child-like reaction associated with rage. Once the distinction between rage and outrage is clearly understood, a person can respond appropriately to situations that create this degree of intensity in emotional response.
When a person's hTMA profile reflects healthy mineral levels and ratios, it shows that adequate energy is available to the neuroendocrine system to enable one to respond to stressors effectively. An emotional response of rage may be a good behavioral indicator of biochemical imbalance. — Editor
Copper Toxicity, and Sodium/Potassium Ratios in Psychological Functioning
There are strong associations between certain psychological functions and essential nutrient minerals that are vital to the production of energy at the cell and tissue level. These nutrient minerals are most easily and accurately measured in a hair tissue mineral analysis (hTMA). It has long been recognized that a person's energy level is strongly associated with one's psychological functioning. Psychic energy was the essence of Freud's "economic" principle in his theory of personality. Psychiatric and psychological definitions of depression have included fatigue or low energy levels as key indicators of this condition.
Most psychodynamic systems postulate an internal psychic conflict as the major factor that drains psychic energy and leads to clinical depression. In these psychodynamic systems, psychic energy is conceived of as a hypothetical construct that is not directly linked to the known physical energy system of the body. The latter involves the intracellular production of energy that is highly dependent on various nutrient minerals and their interrelationships. Current bio-psychiatric theories postulate biochemical imbalances affecting neurotransmitters as the "causes" of depression. These theories often turn out to be nothing more than rationalizations for prescribing powerful toxic psychotropic medications (Breggin, 1991).
SPECIAL REPORT - Psychiatric drug-induced Chronic Brain Impairment (CBI): Implications for long term treatment with psychiatric medication
Report author: Peter R. Breggin, Director of the Center for the Study of Empathic Therapy
Report author Dr. Breggin discusses the hazards associated with long-term exposure to psychiatric drugs. Drawing on the scientific literature and clinical experience, he describes the syndrome of Chronic Brain Impairment (CBI) which can be caused by any trauma to the brain including Traumatic Brain Injury (TBI), electroconvulsive therapy (ECT), and long-term exposure to psychiatric medications.
In psychiatric practice, these hypothetical biochemical imbalances are not tested or measured in any way either for the initial diagnosis or to assess change over time. These biochemical imbalances are simply assumed and then "proven" to exist by the empirical "effect" of a particular medication on the patient. In 1977, Dr. John Cooper introduced me to the concept of the Judge in clinical psychological practice (Cooper, 1977). For Cooper, the Judge is a phenomenological entity that embodies all of the pathological characteristics of the Freudian superego and none of its healthy qualities. The Judge in Cooper's view is intrinsically an anti-life force. It is inherently a major stressor in a person's life. As the Judge develops in the child from the "should's" and "should nots" of the significant adults in the child's life, the Judge tends to take on a tangible or symbolic form. This visual or symbolic form also encodes judgmental messages along with a very threatening aura. Thus, when the Judge is triggered in the child, adolescent, or adult, the "fight or flight" stress response results. Fear, sweaty palms, muscle tension, racing or pounding heart, etc. are experienced. Conversely, stress itself can trigger a flare-up of one's Judge psychologically. Depending on whether a person identifies with the Judge in the significant adult and becomes the Judge, or whether the person remains a vulnerable target of the Judge, the dominant emotional stress response will be determined. The person who becomes the Judge will attempt to control and dominate others by threats and anger. Such a person operates from the "fight" part of the "fight or flight" response. Such a person usually will be a very determined and decisive person. He/she will often treat others in a very cold, unfeeling, insensitive manner.
On the other hand, the person who remains the vulnerable impotent victim of the Judge will most likely respond from the "flight" part of the "fight or flight" stress response. Fear and panic will be the major responses of this individual. They will often be tentative and indecisive, plagued by doubts. Such a person may also be highly distractible.
The fundamental stress response involves psycho-physiological biochemical changes including glandular, hormonal, and mineral changes. One of the changes involves the activation of the adrenal glands leading to an increase in the secretion of the hormone aldosterone that raises sodium levels in the body's tissues. A high hTMA sodium level also tends to be related to feelings of anger. The higher the sodium level, the more likely the person will experience feeling anger, especially when the sodium level is much higher in the body's tissues than the potassium level. This is illustrated in figure 1.
Na/K Fight or Flight
Scale = Number "1" represents the ideal level for that mineral.
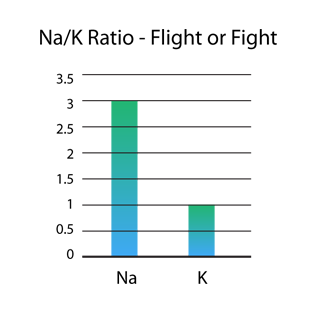
Figure 1. The sodium (Na) level shown here is three times greater than the potassium (K) level. In clinical practice, a high ratio of sodium to potassium is usually a reliable indicator of anger. If a person were overtly angry with a high tissue sodium/potassium ratio, it would be expected that such a person would tend to behave from the "fight" position. They would tend to control and manipulate by threat and anger.
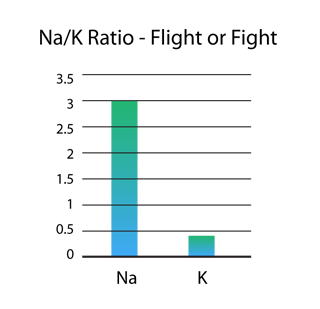
Figure 2. An even greater extreme version of this angry Judge-dominated person can be seen in figure 2, where the Na level is more than six times greater than the K level. In this example, the emotional reaction may intensify from anger to rage.
In contrast, the person who experiences the Judge from the victim position would usually operate from the "flight" part of the stress response. Such a person would easily be overcome by fear and anxiety (Fig. 1). They would feel overwhelmed and impotent to combat the threat of the Judge. Avoidance behaviors or becoming immobilized would be the dominant behavioral responses to the Judge. If the person has a much higher hTMA Na/K ratio as in Fig. 2, panic attacks and phobic behaviors may develop. Obsessive-compulsive thoughts and behaviors may characterize such a person. Deceitful and lying behaviors would also be used to avoid a confrontation with the Judge. Emotions would be turned inward because it would be dangerous to show one's feelings, especially negative feelings to a Judge-dominated person.
The ratio of sodium to potassium in a hair tissue mineral analysis (hTMA) may be a useful index of the person's personality tendency. Although an individual may have a dominant emotional stress response mode, under certain stress conditions an opposite mode of response may occur. The high sodium/potassium individual may tend to respond primarily from the "fight" position with threats and overt anger, but on occasion it would still be possible for such a person to also respond from the "flight" mode in reaction to stress. In the person whose dominant mode of response to stress is anxiety, the individual may "lose it" and explode with anger.
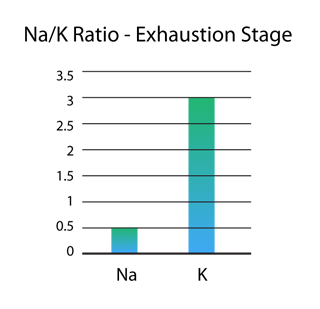
Figure 3. Na/K Ratio - Exhaustion Stage. This figure represents a sodium/potassium inversion, indicating the exhaustion stage of stress.
A tremendous amount of energy is required to turn emotions inward and to suppress them. This leads to an energy drain and to a depletion of the adrenal glands. When this occurs over time, the adrenal glands are no longer capable of secreting adequate amounts of aldosterone in order to keep the sodium level in balance with potassium. Under such conditions, the tissue sodium level drops below the level of potassium, creating an inversion of the ratio of sodium to potassium shown in figure 3. When a person has this inverted ratio of Na/K, they tend to have difficulty making important decisions and may be prone to procrastination. This serves to psychologically avoid a confrontation with the Judge in regard to making a decision. The person is afraid that, no matter what they decide, the Judge will say it's wrong. Finally making a decision often results in relieving tension and freeing a great deal of bound up energy. Often, the very making of a decision helps initiate a correction of their Na/K inversion.
For the individual who is in a Na/K inversion and tends to react with the "flight" mode of response to the Judge, an empathic psycho therapeutic approach involving a direct confrontation with the Judge is often necessary. This helps to reduce the terror of the Judge's threats and to remove the emotional block to a stronger adrenal response to stress. In order for such an individual to move out of a chronic sodium/potassium inversion, it is often necessary to first obtain emotional relief before a strengthening of the adrenal glands will occur, allowing for an increase in the hTMA sodium level.
Other individuals, when placed on a hTMA corrective nutritional program, will experience sufficient adrenal strengthening to be able to make the necessary life choices and changes. The mobilization of increased energy allows the individual to directly face self-judgmental conditioning and reduce its power and control over their emotions.
Copper and Psychology
The mineral copper also plays a significant role in psychological functions and dysfunctions. Copper is unique in that, nutritionally, it is vital for many normal metabolic processes including energy production in the cells and tissues. However, in excess, copper can become extremely toxic and lead to severe mineral imbalances with their corresponding psychological and physical dysfunctions. Copper toxicity has been observed in association with major psychological problems including hyperactivity, depression, attention deficit disorder, memory problems, anxiety and panic attacks, violence, and emotional deadness.
Copper has a strong relationship to calcium and to potassium. As copper increases in the cells and tissues, calcium also tends to rise; potassium tends to drop. hTMA research has shown that copper is involved in the regulation of these other two vital nutrient minerals. As hTMA calcium rises in the cells and tissues to a level substantially beyond its optimal level, it tends to reduce energy production by slowing the activity of the thyroid gland. Such a buildup of calcium will also tend to block feelings as well as energy production. Therefore, anyone who becomes highly copper toxic will begin to experience a deadening of feelings. Similarly, when potassium is significantly reduced relative to sodium (a high Na/K ratio), then hostile, angry feelings will tend to increase. Other individuals will become more and more anxious and fearful. Some people may experience panic attacks. Thus, with increasing copper toxicity, there may be a tendency towards colder, judgmental, unfeeling reactions accompanied by a substantial amount of anger and/or anxiety and fear. Such an individual would be likely to show a mineral pattern involving a high calcium/magnesium ratio and a high sodium/potassium ratio. High copper and/or a low zinc/copper ratio may be seen in the tissue mineral analysis profile. This type of hTMA profile is illustrated below in Figure 4.
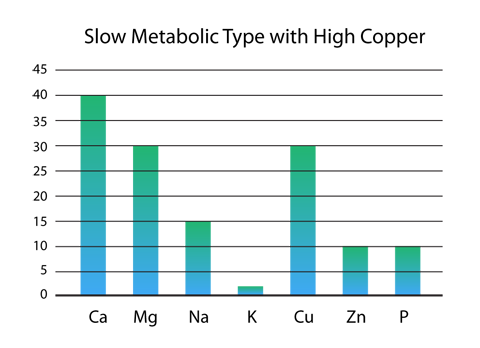
Figure 4. Slow Metabolic Type with High Copper. The same basic mineral pattern may also be generated when a person identifies with the Judge and operates from the "fight" mode of the stress response with intense manifest anger. Such an angry mode of response will tend to increase sodium in the tissues relative to potassium. As sodium increases, magnesium tends to fall in the tissues. Again, a high calcium/magnesium ratio and a high sodium/potassium ratio will result.
Some individuals may have large amounts of copper that are tightly bound up in cell and tissue storage. This will usually appear as a low hTMA copper level. With copper in such a bio-unavailable state, the potassium level may rise significantly above the sodium level, thus creating an inversion of the sodium/potassium (Na/K) ratio (see Fig. 3). This will reflect a tendency towards inhibition, indecisiveness, and suppression of anger with anxiety breaking out.
The reverse process may also occur psychologically. The person who tends to suppress anger does so by also suppressing their adrenal response. This process will slow down the metabolic rate and allow more copper to rise in the tissues (see Fig. 4).
Another characteristic strongly associated with an extremely high hTMA copper level is fear, anxiety or panic. Problems with personal boundaries are commonly observed in individuals with high hTMA copper levels because their sense of awareness seems to be impaired. Fear, panic and terror may increase in people with high hTMA copper, especially under intense stress. Under stress, zinc tends to be lost from the body's cells and tissues. When this occurs, the individual may experience a high copper condition because the zinc/copper ratio is lowered. If such an individual also has unresolved emotional issues, under high stress conditions the person may experience a feeling of being in danger, without awareness of what is happening psychologically.
Fear and terror may break through and be felt for no apparent reason. This may further exacerbate the stress that triggered the loss of zinc and induced the attack in the first place. With continued stress, the impact may continue to intensify. In extreme cases, suicidal hopelessness and depression may be felt with intense feelings of doom. The person may feel that there is no escape from these awful feelings. The optimal treatment for such a copper toxic condition involves the combination of nutritional supplementation and empathetic therapy. The primary nutrients that help to reduce the effect of copper toxicity (see Fig. 4) are zinc, vitamin C, vitamin B6, magnesium, and potassium. Since most people are able to bring up an image of the Judge, guided imagery and art therapy are well suited for the therapeutic process of "shrinking" the Judge.
Back to TopPersonality Characteristics Reflected in hTMA Patterns1
D. L. Watts, Ph. D.
The endocrine and nervous systems' response to stress, either physical or emotional, is well known and has been described in the "fight or flight" mechanism. As stated by Dunbar, "It has been said that the endocrine glands translate the tempo of the nervous system into the tempo of metabolism and vice-versa. But sometimes the glands are the pacemakers for emotion ..." Emotions can trigger endocrine responses, which in turn affect nutritional status. Studies have shown that the emotional status of an individual can affect the absorption and excretion of minerals. Henkin reported that "Trace metals have been shown to influence hormones at several levels of actions … Similarly, hormones have been shown to influence trace metal metabolism … including excretion and transport."2 3 4
Since it is well known that psychic factors can trigger an increase in mineral excretion and/or absorption, it is reasonable to assume that chronic emotional stress may be reflected in hTMA patterns.
The relationship between mental disorders and mineral patterns through tissue mineral analysis of hair is in its early stages of research. Thus far hTMA research has revealed significant findings on the relationship of toxic heavy metals such as lead, mercury and cadmium as well as other nutrient elements. Blood and hair levels of lead have been correlated with continuing exposure in individuals who are occupationally exposed. However, since heavy metals normally depart from the blood stream for deposition into tissue, blood levels do not accurately reflect past exposures. This has been illustrated in studies of children with former lead exposure. Alterations in central nervous system functions are found to be present even when the serum level of lead is well below the upper limits of 30 mcg per dl. Therefore, hTMA is probably the most valuable screening tool for assessing previous heavy metal burdens.5 Toxic metal exposure occurs in utero, and hTMA has been found useful in assessing maternal exposure in neonate hair.7 8
Observation of thousands of hTMA patterns over many years has led to the recognition of associated personality traits. In order to simplify this discussion, the categorization of individuals according to hTMA patterns will be reviewed. Eight distinctive hTMA patterns are identified as sympathetic types 1 through 4 and parasympathetic types 1 through 4.
Categorization of nutrients including vitamins, minerals, foods and drugs into sympathetic and parasympathetic categories has been reported elsewhere. The sympathetic type 1 is considered to have an elevated metabolic rate and a relative increase in the tissue retention of sympathetic minerals, which include phosphorus, sodium, potassium and iron. The parasympathetic type 1 has a reduced or sedated metabolic rate with a relative increased tissue retention of parasympathetic elements calcium, magnesium and copper. The subtypes have variations of sympathetic and parasympathetic mineral retention.
- Aggressive Behavior
-
William Walsh was probably the first researcher to report the correlation of hTMA patterns to aggressive or violent behaviour.9
He reported significant hTMA mineral variations in subjects who had committed violent crimes compared to those who were less violent. We have found that elevated tissue sodium and potassium levels are related to aggressive personality traits, particularly in the sympathetic type 1 individuals. hTMA patterns of sympathetic types show low calcium/phosphorus (<2.63) and calcium/potassium (<4.0), and elevated sodium/magnesium (>4.0) ratios. The sympathetic type 1 is analogous to the type A personality: highly competitive, aggressive, constantly in a hurry and easily angered or hostile.
The elevated tissue sodium and potassium levels in sympathetic types can be clinically associated with increased adrenal and thyroid activity. Aggressive behavior is associated with hyper adrenal conditions such as Cushing's syndrome, as well as induced hyper adrenal states due to the use of corticosteroid therapy. Increased sympathetic neuroendocrine activity contributes to the retention of sodium and potassium, which helps to explain the increased incidence of heart disease in the sympathetic types.
Elevated tissue iron is also associated with hostility. This is perhaps due to the accumulation of iron in the hippocampus region of the brain. Excess iron accumulation can affect neurological function by increasing lipid peroxidation or by displacing other minerals normally present in the region of or within the hippocampus. Hyperactivity is often seen in children with elevated tissue iron levels.
- Anxiety
-
Aggressiveness, hyperactivity and anxiety are all associated with the sympathetic type 1 pattern, which is associated with low tissue calcium and magnesium relative to sodium and potassium. Decreased tissue calcium is associated with neuromuscular hyperexcitability. Many symptoms of anxiety neurosis are identical to those seen in patients with hypocalcemia.6 Patients suffering from anxiety neurosis show excessive serum lactate levels. Lactate infusion, which readily brings on anxiety symptoms in patients, can be prevented by calcium infusion. Apparently the mechanism behind anxiety neurosis is over activity of the central nervous system and adrenal function, both of which increase calcium and magnesium losses from the body and increase tissue retention of sodium, potassium and phosphorus.
- Addiction
-
hTMA patterns suggest that it is important to make a distinction between physiological and/or psychological addictions.
A physiological addiction is associated with the sympathetic type 1, which is analogous to Watson's "fast oxidizer."10 Their metabolic machinery is in high gear, so to speak, which requires constant fueling. In review, their hTMA pattern is dominant in the stimulatory minerals, phosphorus, sodium, potassium, etc., which indicates a high rate of metabolism and sympathetic neuroendocrine dominance. In order to keep their high level of energy, they may develop addictive personality reactions to stress such as being late for appointments, waiting until the last minute to meet deadlines and starting several projects at once. This stress continuously stimulates the neuroendocrine system, which in turn helps to maintain their high energy levels. The result of this type of behavior if left unchecked is ultimately the "burnout syndrome." We have found that the sympathetic type 1 is often found to have a strong allergy or sensitivity to grains, which leads to an addiction, frequently to alcohol. The grains lead to increased losses of calcium and magnesium with increased retention of phosphorus, sodium, potassium and iron.
Psychological addiction is seen in parasympathetic types, which are analogous to Watson's "slow oxidizer." Due to the sedative mineral and parasympathetic neuroendocrine dominance, decreased energy production is evident. Along with this biochemical pattern, fatigue, depression and low self-esteem can develop. In an effort to feel better generally and psychologically, they may yield to food cravings such as binging on refined sugars and carbohydrates in order to increase their energy levels. Eventually the use of recreational chemicals or alcohol may develop due to their immediate energy-elevating and mood-altering effects.
- Mania and Depression (Bipolar)
Generally speaking the sympathetic type 1 pattern has been observed in patients with manic-depressive illness. It has long been known that manic and excited paranoid patients have increased rates of neurotransmission while depressed patients have a decreased rate of neurotransmission. Increased membrane permeability at the synaptic level is associated with increased sodium retention. Studies have reported that adrenal hormones fluctuate concomitantly in patients experiencing manic-depressive cycles and depression. 11 12 13
Such disorders are more specifically related to the sodium-to-potassium ratio. Diagnosed manic depressive patients usually show an elevated tissue sodium and potassium but a much lower sodium/potassium ratio. Manic depression is more frequently found in patients who are sympathetic dominant with elevated thyroid (Type I and 3). A report in the "New England Journal of Medicine," June 30, 1988 stated that neuropsychiatric disorders due to cobalamine deficiency can commonly occur in the absence of anemia and that improvement is frequently noted with cobalamine therapy.
We find that the thyroid is elevated in patients with manic depressive disorders. Lithium, a mineral used for many years in the treatment of manic depression, has been proven helpful in controlling these symptoms. Lithium is known to suppress thyroid activity, which could also be the mechanism behind its effects. In addition, cobalt and vitamin B12 are thyroid inhibitors, which could also explain their beneficial effect upon neuropsychiatric disorders. This may explain the mechanism behind the effectiveness of lithium in that lithium salts temporarily improve the metabolic ratio of these electrolytes.
- Depression
-
Depression is commonly seen in the parasympathetic types. The hTMA pattern consists of elevated tissue calcium and magnesium levels relative to phosphorus, sodium and potassium. This pattern is associated with adrenal and thyroid insufficiency, a condition which contributes to a reduction in metabolic rate and energy production.
Exhaustion is an aspect of depression that occurs alone or in combination with other symptoms, including anxiety, fear and sadness. As mentioned previously, hypercalcemia is universally associated with depression. Increased magnesium levels have similar effects as calcium. Sodium deficits are related to abnormalities in membrane permeability. Lowered membrane permeability is associated with decreased synaptic impulse transmission and has been found in underactive or depressed groups. Fluctuations in adrenal steroids have also been noted in patients during mood alterations.7 In addition hypothyroidism has been noted in affected patient groups compared to normal control groups.14 15 16
Conclusion
This article discusses a few of the clinical hTMA observations made between personality and tissue mineral patterns. Further development of hTMA in this area may help to uncover more relationships between emotions and disease. Most disease conditions have an emotional counterpart. It is recognized that emotions are linked to biochemical changes which can lead to the development of disease. For instance, the relationship of Type A behavior with an increased incidence of heart disease.
Emotional factors trigger an increase in mineral excretion and absorption. Chronic or strong emotional reactions produce neurological, hormonal and ultimately dynamic nutritional changes, which will eventually lead to metabolic changes that can be measured. For example, an increase in circulating stress hormones, as well as changes in mineral concentrations, will be reflected in a hTMA. Tissue mineral patterns reflect these changes. hTMA may prove an to be a valuable clinical tool for assessing psycho-somatic and somatopsychic relationships.
- hTMA Mineral Ratios Brief discussion of their importance.
Resources
Related
- Brain-Altering Psych Drugs and the "Batman" Shooter Gary G. Kohls, MD
Download
Video
- Reason behind many mass shootings and random violence
- Violence - David Healy.org Drugs sometimes cause people to have violent acts thoughts and behaviour. These may include thoughts of suicide or harming others. These videos explain how this can happen.
- Trace Amounts Official Trailer. Autism and vaccines.
Website
- Rx Risk.org pharmaceutical risk education and information
- Children's Environmental Health Network
- Aaron Swartz
- Suicide.org
Book
- The Hacking of the American Mind Robert Lustig, MD
References
Malter References
- Cooper, J. personal communication, 1977.
- Breggin, P. Toxic Psychiatry: Why Therapy, Empathy, and Love Must Replace the Drugs, Electroshock and Biochemical Theories of the "New Psychiatry." New York, St. Martin's Press, 1991.
- Malter, R.F. "The concept of the Judge in the diagnosis and treatment of emotional problems." American Psychological Association, Washington, D.C., 1982.
- Malter, R.F. "Nutritional concerns in learning and psychological disorders." Paper presented to APA Div. 42, annual convention of the American Psychological Association, Los Angeles, CA, August, 1985.
- Malter, R.F. "Trace mineral analysis and psychoneuroimmunology." Journal of Orthomolecular Medicine, 2nd quarter, vol. 9, no.2, 1994, 79-93.
- Malter, R.F. "Trace mineral analysis and psychoneuroimrnunology." Townsend Letter for Doctors & Patients. Port Townsend, Washington, April, 1996.
- Malter, R.F. & Malter,R. Shrinking the Judge: Freeing the Inner Child. Education & Health Resources, Hoffman Estates, Illinois, 1996; 1998.
- Malter, R.F. "Stress Related Disorders and Tissue Mineral Analysis (hTMA):The Mind/Body Connection" American Psychological Association, Mid-winter convention, St. Petersberg, FL, 1997a.
- Malter, R.F. "Beyond cognitive behavior therapy: the power of imagery in psychotherapy." American Psychological Association, Mid-winter convention, St. Petersberg, FL, 1997b.
- Malter, R.F. "Stress Related Disorders and Tissue Mineral Analysis (hTMA):The Mind/Body Connection" American Psychological Association, Mid-winter convention, La Jolla, CA, 1998a.
- Malter, R.F. "Beyond cognitive behavior therapy: the power of imagery in psychotherapy." American Psychological Association, Mid-winter convention, La Jolla, CA, 1998b.
- Malter, R.F. "Preventing postpartum depression: a case report." Journal of Orthomolecular Medicine, 4th quarter, vol. 16, no.4, 2001, 213-217.
- Watts, D. L. Trace Elements and Other Essential Nutrients: Clinical Applications of Tissue Mineral Analysis. Trace Elements, Inc., Dallas, Texas. 1995.
- Malter, R.F. "The Influence of "Junk" Science in Manipulating and Shaping the Healthcare Marketplace" Journal of Orthomolecular Medicine, 2nd quarter, Vol. 16, No.2, 2001, pp 91-93.
- Watson, George. Nutrition and Your Mind. New York: Harper & row, 1972.
Watts References
- Trace Elements and Neuropsychological Problems as Reflected in Tissue Mineral Analysis (hTMA) Patterns. David L. Watts, Ph.D., F.A.C.E.P., Journal of Orthomolecular Medicine Vol. 5, No. 3, 1990.
- Dunbar F: Mind Body: Psychosomatic Medicine. Random House, N.Y., 1955.
- Hathaway ML: Magnesium in Human Nutrition. U.S.D.A. Wash. D.C., 1962.
- Henkin RI: Trace metals in endocrinology. The Medical Clinics of North America. 60, 4. Burch, R.E., Sullivan, J.F., Eds. W.B. Saunders, Phil., 1975.
- Kopito L, et al: Chronic plumbism in children.
- Pitts FN: The biochemistry of anxiety. Scientific Am., Feb. 1969.
- Baumslag N, et al: Trace metal content of maternal and neonate hair. Arch. Env. Hlth. 29, 1974.
- Huel G, et al: Increased hair cadmium in newborns of women.
- Ralaff J: Locks — A key to violence. Sci. News 124, 1983. Am., Feb. 1969.
- Watson G: Nutrition and Your Mind. Harper and Row, N.Y. 1972.
- Stevens JD: Membrane permeability in schizophrenia. Dis. Nerv. Sys. 25:21, 1964.
- Bunney WE, et al: Study of a patient with 48-hour manic-depressive cycles. Arch. Gen. Psychiat. 12, 1965.
- Bunney WE, et al: Correlations between behavioral variables and urinary 17-hy-droxycorticosteroids in depressed patients. Psychosom. Med. 27, 1965.
- Gibbons JL, McHugh PR: Plasma Cortisol in depressive illness. /. Psychiat. Res. 1, 1962.
- Bunney WE, et al: Correlations between behavioral variables and urinary 17-hy-droxycorticosteroids in depressed patients. Psychosom. Med. 27, 1965.
- Simpson GM: Thyroid indices in chronic schizophrenia. /. Nerv. Ment. Dis. 137,1963.
Editor's note: This article may or may not contain minor editing from the original document. Editing is done for one or more reasons: technical issues, layout or space considerations, content accuracy and/or clarity. © Copyrighted content is owned by the author. Please contact the author if you have any questions or would like to use any of their content for any reason whatsoever. Thank you.