Update: 03 December 2024
Dental Health
Author: Julie Casper, C. Ac.
"The mouth is a mirror of health or disease, it is a sentinel or early warning system, the mouth provides an accessible model for the study of other tissues and organs, and it's a potential source of pathology affecting other systems and organs."
— Oral Health in America: A Report of the Surgeon General
Contents
- How to Improve Dental Health
- Visit Your Dentist Regularly
- Root Canal Therapy (RCT) (endodontic treatment)
- Dental Amalgams
- Detoxification Methods
- Resources
- References
How to Improve Dental Health
Dental health is an appreciable indicator of overall health status. It is the result of good dental hygiene practices, and an individual's biochemical balance.
Prevention is the only true solution to dental health problems. A dental carie (cavity) often indicates a mineral imbalance and an under functioning immune system. The only science-supported way to prevent tooth decay is by practicing good oral hygiene, and by ensuring that your mineral levels are adequate and their ratios are properly balanced (i.e., good general health).
It is discouraging and frustrating to see such an enormous expenditure of money and technology just to keep alive the fiction that diseased teeth are inevitable; and that the only person who can do anything about disease damage is a dentist with his mechanical tools. Robert O. Nara, DDS
- How to Become Dentally Self-Sufficient Robert O. Nara, DDS
- Money by the Mouthful Robert O. Nara, DDS
In a 1934 article titled: "Metabolic Disturbances in Relation to the Teeth," Charles Brödeker, DDS, explains the importance of the proper balance of essential minerals to dental health.
Unfortunately, the decline of your dental health often starts at the dentist. In conventional dentistry, when a tooth's structure is compromised by drilling to repair a cavity, a cascading cycle of failure begins, or "death spiral" which ultimately ends with the death of the tooth.
Mercury amalgams (metal silver fillings) are toxic, and as these fillings age, they corrode, expand and crack teeth. When a tooth that's been drilled and filled cracks, a dentist typically will recommend a potentially lethal treatment — the root canal.
Conventional dentistry's repair-replacement-repair cycle is expensive! It is estimated that each tooth will end up costing, on average, more than $2,800 in dental repair services by the age of 79. And the lifetime cost of the failing tooth increases when it requires a root canal, extraction or replacement with a prosthetic.
Source: The true cost of a cavity. When a little hole becomes a 2,000 dollar money pit. Dent. Today. 2004; Oct 23(10):70.
Dental Health and the Hypothalamic-Parotid Axis
Research published in the 1970s by Ralph Steinman D.D.S., and endocrinologist Dr. John Leonora, examining the role of dentinal fluid flows in the teeth of rats found that early hypomineralisation of the enamel and subsequent decay were related to dentinal fluid flows in rats fed a tooth decay promoting diet. And, that systemic administration of urea and citrulline could reverse caries. Their findings support the hypothesis that tooth decay is a systemic metabolic issue produced by disruption to the hypothalamic-parotid axis caused by the diet. The nutritive composition (i.e., diet) thus proved to be critical for the secretion of the parotid hormone. Nutritive substrates activate neural stimuli going to the hypothalamus, which in turn activates the hypothalamic-parotid gland endocrine axis that then stimulates the dentinal fluid transport mechanism.
The hTMA lab report provides information that can identify the status of your hypothalamic-parotid axis. You can then improve your ratios of essential nutrient minerals to support healthy endocrine function.
Another group of investigators at the University of Oulu Dental School, Oulu, Finland, Tjaderhane, L. et al., (1994) studying the formation of dentin, discovered that the parotid hormone not only regulates the flow of dentinal fluid but also is involved in the formation of dentin — dentinogenesis. In addition, they discovered that a high sucrose diet in young rats suppressed primary dentinogenesis. The injection of carbamyl phosphate significantly reversed the effect of sucrose — but only in intact rats. Furthermore, carbamyl phosphate prevented the atrophy of the parotid glands associated with the ingestion of sucrose.
Gum Disease
The early stages of gum disease are usually painless so can be unnoticed. Degenerative gum disease actually includes several oral diseases that develop slowly over years. These diseases affect the gums, jaw bone and other supporting structures of the teeth. Oral diseases not treated in time can lead to painful, bleeding gums, oral infections, and eventually tooth loss.
Healthy Gums are firm and resilient, with a nice pinkish color. Healthy gums do not bleed on probing. The tissue is firm with a normal variation of lighter and darker areas. If you allow plaque to build up between your teeth and gum line, it leads to the build up of tarter and calculus. This causes bad breath, unsightly teeth, and it is the primary cause of gum disease.
Calculus and tartar are different names for the same substance that comes from the second stage of plaque accumulation where the bacterial film begins to harden. The development of tartar (calculus) leads to rapid tooth decay, and increases the severity of gum infections. Tartar needs to be removed through a special procedure by a periodontist, followed by special care to allow your gums to heal. Do your best to avoid the accumulation of plaque, and the development of tartar (calculus) by practicing proper oral hygiene and receiving routine tooth cleaning procedures from your dental hygienist.
Progressive Stages of Degenerative Oral Disease
- Gingivitis: An inflammation of the gingiva or gums with a loss of color variation. Gum tissue is red, inflamed and bleeds when probed or when brushing. Puffy tissue causes shallow pockets between gum and tooth.
- Early Periodontitis: Marked by loss of gum attachment and a slight loss of bone. Bleeding is more persistent on probing. Pockets of 34 mm develop between teeth and gums in one or more areas of the mouth. There can be a sense of vague aching, pressure and/or itching in the gums.
- Moderate Periodontitis: Supporting gums and bones have deteriorated and teeth may start to loosen. Horizontal bone loss is suffered up to 1/3 of the length of the tooth root. The gum attachment to the tooth weakens and pockets are now 46mm deep. Teeth may look longer, as gums begin receding. Bad breath becomes noticeable.
- Advanced Periodontitis: Tissue and bone are destroyed causing tooth loss. Pockets are now more than 6mm deep with considerable bleeding upon probing. Eating is difficult and painful and teeth may be sensitive to hot and cold. Bad breath is constant and general health may be affected.
- Relationship of Fluid Transport Through the Dentin to the Incidence of Dental Caries Ralph Steinman, DDS
- What is Dental Decay? Robert Gammal, BDS
- Overview of Dental Pulp: Functions and Responses to Injury Australian Dental Journal
The Ideal Oral Health Routine
It's amazing that most of us don't have a correct preventive routine, because it' the most influential thing we can do ourselves to preserve our teeth. And it's easy! Invest about 10 minutes 2 TIMES daily to help prevent plaque from gaining a stronghold and have a great smile for life. Some of the tools used and the order of the tasks may be different than you are used too, here are the basics:
Tools Needed:
- Soft-Bristle toothbrushes (use 2 so they can dry between uses)
- Dental Floss
- Interdental Brushes
- Water irrigator
Perform twice daily, preferably first thing in the morning (before breakfast) and last thing before bed. In addition to cleaning the goal is to disrupt plaque formation.
- Floss (correctly, remove plaque from sides of teeth).
- Brush between teeth with Interdental Brush (tooth spacing may require different diameter sized brushed).
- Carefully brush only two teeth at a time and pay very close attention to how proper technique feels. Angle the brush into your gum line and use gentle motion to disrupt plaque colonization. Start at the back (lower left outside surface) and work you way systematically around to the other side. Switch to the top back outside surface and work you way back again. Then do the same pattern with the inside surface gum line. Next do all the tooth surfaces with a brisk sweep action (from bottom to top). Finally, brush chewing surface tops with a gentle circular motion.
- Rinse along the gum line with an Oral Irrigator. The importance of gum line irrigation cannot be understated and provides exceptional therapy for insuring healthy gums.
- The Ideal Oral Health Routine A comprehensive HOW-TO guide.
- Correct Toothbrushing Technique Scott Frey, DDS
- How to Floss ADA
It's important to thoroughly and gently brush your teeth using a soft bristle tooth brush and nontoxic toothpaste. The FDA requires most toothpaste include a poison warning label, and today some products contain plastic particles. Some floss products contain forms of perfluorochemicals (PFC's) which are linked to enhanced tumor growth and cancer. Try to purchase natural, toxin free floss varieties which may contain vegetable waxes, pure essential oils for flavoring and do not contain PFC's. Also, most flosses are made of petroleum-derived nylon, the better choices avoid petroleum-based paraffin wax in favor of nontoxic beeswax, carnauba wax or jojoba wax.
Stained teeth? If the staining is from coffee or tea and you don't want to give them up, you can reduce staining by adding a little full-fat milk or cream. The dairy fat provides a kind of protective coating. It must be real dairy though. No synthetic substitutes, or nut milks — and never use soy milk for anything. Avoid chemical teeth whitening products and procedures. Diet choices and a good hygiene routine are the best way to maintain a great smile. Artificial teeth whitening products have been found to contain coal tars, fluoride, aspartame, aluminum, benzene and other toxic components that can harm tooth enamel, gums and your overall health. The trays and strips that hold the whitening solution also can leach toxins into your body.
Back to TopVisit Your Dentist Regularly
An annual visit to an open-minded dentist and/or a dental hygienist for inspection and cleaning is a good preventive measure. However, some conventional dental practices and procedures cause serious harm and should be avoided (e.g., root canal, drilling, amalgam filling, x-ray, etc.).
When possible, resist x-rays unless absolutely necessary. For one thing, x-rays are very difficult to interpret correctly, even for an expert radiologist. The cancer causing effects of ionizing radiation from an x-ray are well documented in the scientific literature. In addition, the definitive dental information that an x-ray is able to show is very limited. For example, it is impossible to demonstrate infection with an x-ray because dental radiographs show hard tissue only. They do not accurately represent soft tissue, or infections. Due to the shadow cast by the root it also may be impossible to see bone loss.
Please select your dentist carefully.
- The Truth About Dentistry (F. Jabr) Dentistry prone to gratuitous procedures.
- Try to find a Biological Dentist.
Silver Diamine Fluoride (SDF)
Silver fluoride has the potential to play an important role in minimal intervention dentistry. If you have tooth sensitivity or a cavity ask your dentist about using SDF. The use of SDF in dentistry to treat dentine hypersensitivity and arrest caries goes back at least fifty years. SDF is inexpensive, non-invasive, and quick and easy to apply. It provides two major clinical benefits:
- Immediate relief from painful tooth sensitivity (generalized dentine hypersensitivity).
- Immediate control of carious dentine. SDF can stop existing carries from further deterioration and even prevent new cavities.
Until now, no option for the treatment of dental caries in the United States besides restorative dentistry has shown substantial efficacy. Silver diamine fluoride is an inexpensive topical medicament used extensively in other countries to treat dental caries across the age spectrum. No other intervention approaches the ease of application and efficacy. Multiple randomized clinical trials – with hundreds of patients each – support use for caries treatment, thus substantiating an intervention that addresses an unmet need in American dentistry. In August 2014 the Food and Drug Administration (FDA) cleared the first silver diamine fluoride product for market, and as of April 2015 that product is available.
Silver nitrate, typically a 25% solution, has been used in the U.S. (including acceptance by the ADA) and in other countries for more than 100 years for arresting dental caries — without incident. In fact, not a single adverse event has been reported to the Japanese authorities since they approved silver diamine fluoride more than 80 years ago (Saforide, Toyo Seiyaku Kasei Co. Ltd., Osaka, Japan). The silver acts as an antimicrobial, the fluoride promotes remineralization, and the ammonia stabilizes high concentrations in solution. Worldwide clinical use has demonstrated the anti-caries effect of silver fluoride.
Silver fluoride/silver diamine fluoride causes black staining. This staining comes from the reduction of silver ions to metallic silver and silver oxide. The FDA approved SDF product Advantage Arrest™ claims it "does not stain sound dentin or enamel" but the UCSF Protocol for Caries Arrest Using Silver Diamine Fluoride lists in it's considerations that decayed dentin will darken as the caries lesions arrest. Most will be dark brown or black. SDF can stain the skin, which will clear in two to three weeks without treatment, and that SDF can permanently stain dental surfaces and clothes.
Being able to paint (SDF) on in 30 seconds with no noise, no drilling, is better, faster, cheaper. Dr. Richard Niederman, the chairman of the epidemiology and health promotion department at the New York University College of Dentistry
Silver diamine fluoride is being used in hundreds of dental offices in the U.S., Medicaid patients in Oregon are receiving the treatment, and at least 18 dental schools have started teaching the next generation of pediatric dentists how to use it.
Benefits of Silver Diamine Fluoride (SDF)
- Non-invasive
- Provides immediate relief from dentinal hypersensitivity
- Stops cavities (dental caries), prevents new cavities
- Hardens softened dentin, improves acid and abrasion resistance
- Kills pathogenic organisms, efficient control of infection. Fillings, by contrast, do not cure an oral infection.
- Easy simple application (paint on)
- Excellent for emergency therapy
- Cost effective
More Information - Silver Diamine Fluoride (SDF)
- A Cavity Fighting Liquid Lets Kids Avoid Dentists' Drills The New York Times
- UCSF Protocol for Caries Arrest Using Silver Diamine Fluoride Excerpt: CDA Journal, Vol 44
- UCSF Protocol for Caries Arrest Using Silver Diamine Fluoride HHS Public Access (J Calif Dent Assoc.)
Root Canal (endodontic treatment)
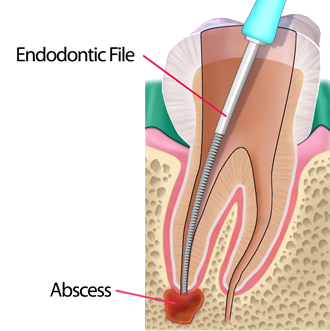
Root canal therapy is a common dental treatment used to resolve tooth pain and maintain mechanical function. Dentists promote it as a way to "save the tooth," but the procedure actually kills the tooth. The actual process removes infected pulp from the inside of a tooth and replaces it with a root filler material. Unfortunately, root canal therapy can have serious negative health consequences.
Dentists are taught that a root canal must be filled to within 1mm of the root apex. The apex of a root canal is only rarely determinable by x-ray. Thus many root canals are worked too short, or too long so that the root filling will protrude through the end of the tooth and into the bone. This is well documented research published in conventional dental literature (e.g., "In the canals which were overfilled, the extruded materials were always associated with advanced destruction of the surrounding tissue and liquefaction necrosis" Malcolm Davis - Periapical and intracanal healing following incomplete root canal fillings in dogs, Oral Surgery, May 1971, Vol. 31 No. 5)
Root canal procedure:
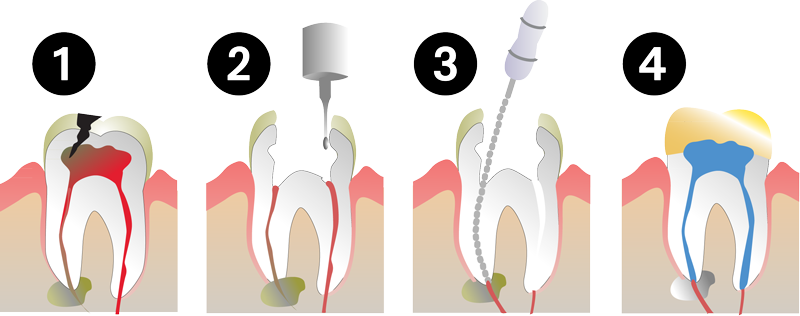
- Infected or cracked tooth.
- Dental surgeon (DDS) drills out an access cavity.
- Dentist removes infected pulp with an endodontic file.
- The open area is sterilized, filled, and sealed with a crown.
A high percentage of chronic degenerative diseases can originate from root filled teeth. The most frequent are heart and circulatory diseases. The next most common diseases are those of the joints, arthritis and rheumatism. In third place - but almost tied for second - were diseases of the brain and nervous system. Dr. George Meinig, DDS
In 2007, the Australian Dental Association published a special supplement to their journal that presents reasons why the root canal procedure does not work. From the publication (paraphrased);
- It is impossible to remove all dead tissue from the tooth. At least 30% of the main canal remains untouched no matter what techniques are used to clean them. The main canal represents the smallest amount of dead tissue in the tooth (most is found in the dentine tubules and accessory canals). Dentine tubules and accessory canals are technically inaccessible. All of the dead tissue which remains in the tooth breaks down and becomes gangrenous and highly toxic (and potentially lethal).
- It is impossible to seal a tooth. All the toxins in the tooth will leach into the body. This includes the materials which are placed in the tooth as part of the procedure ‐ materials that are either cytotoxic (they kill cells) or carcinogenic (they cause cancer).
- Some root canal cements (filler material) are neurotoxic and may cause permanent nerve damage. Many contain formaldehyde that is both allergenic and causes cancer. Root filling cements break down releasing many toxic substances — formaldehyde, ammonia, carbon monoxide, carbon dioxide and toxic sodium oxide, amines, calcium tungstate, zirconium oxide, silica, silicone oil.
Aqueous sodium hypochlorite (bleach) solution is widely used by dentists during root canal treatment. Although regarded by the dental industry as being safe, potentially severe complications can occur when bleach comes into contact with soft tissue. For more information:
The fundamental aim of the root canal procedure is to sterilize the tooth. In the early 1920s Weston Price, DDS, was head researcher for the National Dental Association (NDA). The NDA was renamed the now familiar, American Dental Association (ADA) in 1922. Dr. Price demonstrated that the only way to sterilize a tooth was to boil it for half an hour. This method, for obvious reasons, is not possible as a therapy. Dr. Weston Price studied the effects of dead teeth and root canal therapy on systemic health. He was able to correlate different disease states with the types of pathology seen around dead teeth. He demonstrated thousands of times, the creation of diseases from non vital teeth. He clearly demonstrated how every belief root canal therapy held by the dental community was based on inadequate scientific research. His findings have been largely ignored by the dental profession.
Dr. Price's research clearly demonstrated the deadly effects of root canal fillings. One of his experiments showed that rabbits implanted with a root filled tooth from a person who had died of a heart attack produced a heart attack in the rabbit within weeks of implantation. This was not only true of heart problems. It was true for many conditions including arthritis, kidney disease, and cancer.

Dr. Weston A. Price DDS [1870 – 1948] was a dentist and medical researcher known for his research on the relationship between nutrition, dental health, and physical health. Price's work is influential today, inspiring the emerging field of biological dentistry.
Dr. Weston Price wrote numerous papers on the role of nutrition on health. For nearly a decade, he traveled and investigated some of the most remote areas in the world where he observed perfect dental arches, minimal tooth decay, high immunity to tuberculosis and overall excellent health in those groups of people who ate their indigenous foods. Dr. Price found that when these people were introduced to foods such as white flour, white sugar, refined vegetable oils and canned goods, signs of degeneration became evident quickly. The consequences included dental caries, deformed jaw structures, crooked teeth, arthritis and a low immunity to tuberculosis, among other conditions. In 1939, Price published Nutrition and Physical Degeneration, which details a series of ethnographic nutritional studies he performed across diverse cultures, including the Lötschental in Switzerland, Native Americans, Polynesians, Pygmies, and Aborigines, among many others. The research materials include some 15,000 photographs, 4,000 slides, and many filmstrips. Photos show the contrast between the dental health of people who ate a traditional diet compared with those who ate a modern western diet.
Dr. Weston Price - Select Books and Research
- Dental Infections - Oral and Systemic
Dr. Price spent 25 years of his career performing research on pulpless and endodontically-treated teeth (root canals). Devotion to his research was motivated by personal tragedy. Dr. Price and his wife lost their only son Donald to complications from an infected root canal, which Price himself had put in. Price went on to write a two volume set (1000+ pages) on the problems of systemic dental infections from root canals. Dental Infections - Oral and Systemic includes a dedication to his son (paraphrased): to Donald, who at sixteen, paid with his life the price of humanity's delayed knowledge regarding these heart and rheumatic involvements.
- Dental Infections - Oral and Systemic - Volume I (1923) 500 pages
- Dental Infections - Oral and Systemic - Volume II (1923) 700 pages
- The Pathology of Dental Infections and Its Relation to General Diseases (1916 presentation at the annual meeting of the Canadian Oral Prophylactic Association, Toronto) 24 pages
Nutrition and Physical Degeneration
- Weston A. Price, MS., D.D.S. First published in 1939, this seminal book startled the worlds of science and nutrition with its documented evidence of primitive populations encountering civilization, adopting modern diets, and finding that their health worsened. It remains essential reading for those concerned with food and health.
In the 1980s, one of the founders of the American Association of Orthodontists, Dr. George Meinig DDS, came across Dr. Price's research and tried to publicize it. Even though Dr. Meinig was highly regarded nationally and internationally, and the recipient of many honors, he too was discredited and marginalized by powerful interests. In an attempt to inform the public, he published: the Root Canal Cover Up
"Knowing the chemistry involved in the occurrence of tooth decay and pyorrhoea (gum disease) is fundamental to the understanding of these two diseases. When tooth decay is present, the acid-base balance is depressed. That means it is on the acid side and the level of calcium is lower than normal. For those who have pyorrhoea, the contents of the periodontal pockets are very alkaline and the calcium level is higher than normal.
Pockets can be the cause of the need for root canal treatment whenever a lateral accessory root canal opens into an infected pocket area, thereby allowing the bacteria in the pocket to be introduced into the tooth through the blood vessels which reside in the root canal."
Dr. George Meinig, DDS, FACD, founder of the Association of Endodontists
To date, the dental profession has not been able find a method or material which will sterilize a tooth while it is in the mouth. The bacteria which live inside the tooth are anaerobic (requiring little to no oxygen). Hundreds of different types of bacteria are found in one dead tooth. These bacteria produce some of the most potent and deadly toxins known to man. The old belief that these bacteria and their toxins will become ‘entombed’ in the tooth, and thus not have access to the rest of the body, is known to be incorrect [Ref; Journal of the Australian Dental Association Endodontic Supplement, Vol 52. No 1. 2007 MAR]. All of these toxins, and the bacteria themselves, escape from the tooth and circulate throughout the body. The circulating bacteria may localize on a new tissue and cause an infection in a distant part of the body. The Australian Dental Association agrees that it is impossible to sterilize a tooth, stating "predictable eradication of bacteria from the root canal still remains an elusive goal."
"In an understandable desire to preserve as many teeth as possible, attempts to maintain the masticatory apparatus and its functions, attempts are often made to save teeth which are in fact lost. There is a widespread conviction that this can be done without risk by the sterile evacuation of the pulp, and then refilling the cavity. For decades, the erroneous belief was held that, after such treatment, the tooth is an isolated, lifeless thing, no longer involved in any of the body's processes. This assumption was originally based on the premise that the pulp cavity had only one orifice to the apex of the root below, and by filling, this opening was sealed. However, the dentinal canal does not end in just one opening; instead, it resembles a tree with many branches which penetrate the tooth's body in all directions.
The finer details of the entire dental structure have been exhaustively studied. They have established that there is a lively metabolic interchange between the interior and exterior of the tooth, and that this two-way process takes place along many thousands of hyperfine capillary canals joining the pulp cavity to the exterior surface of the tooth.
Very careful conservation measures may possibly seal off the vertical central-medial-tube of the dentinal canal, but it will never reach the lateral ‘twigs’ branching off from this tube. Nor can it ever close off the innumerable capillary canals. Some protein will always remain in these secondary spaces. If this protein becomes infected, toxic catabolic products will be produced, and conveyed into the body.
It was established in 1960 by W. Meyer (Gottingen) that within devitalized teeth, the dentinal canals and dental capillaries contain large microbial colonies. The toxins produced by these microbes in a tooth with a root filling can no longer be evacuated into the mouth, but must be drained away through the cross-connections and unsealed branches of the dentinal and capillary canals into the marrow of the jawbone. From there, they are conveyed to the tonsils, and thus the flowing systems of the body. In fact, the root canal treatment may literally convert a tooth into a toxin producing ‘factory.’ It then may be left to develop its devastating effect on the organism for decades or even for a lifetime."
Josef M. Issels, M.D., (November 21, 1907 – February 11, 1998)
Root Canal Failure - Tooth Necrosis and Focal Infection
The growing popularity of root canal procedures is surprising because the industry also acknowledges that there is a high statistical likelihood of root canal failure. According to the endodontic industry media, root canal procedures are on the increase, due to;
- Improved techniques make root canal surgery less painful than in the past.
- Root canal therapy is now accepted by more insurance carriers.
- "The dental profession's very successful, long-term public education campaign."
Several factors can result in RCT failure, including the complex anatomy of the root canal system. It is a recognized fact that it is impossible to completely sterilize the endodontic site. Therefore, root canal therapy cannot be 100% guaranteed (officially; 10 – 15% failure rate). Statistically, the failure rate for root canals is much lower for endodontists (5%) than for a general dentist (10-15%, officially). Besides those failures due to missed canals, incompletely treated canals (short treatment due to ledges), complex anatomy, the clinician's lack of experience or the dentist's lack of attention to quality, remaining infected tissue, and bacterial post-treatment leakage — root treated teeth are actually dead, thus weaker than living teeth (also, the body rejects necrotic tissue). A dead tooth carries the additional recognized risk of fracturing under pressure. Even root treated teeth that are reinforced with posts to support either crowns or bridges, carry the risk of fracture and infection.
Officially, industry denies that root canal treatment can be linked to any illness. It is difficult to connect root canal therapy to focal infection and other health problems which can take time to become pathological. Yet, more than 60 years ago, the ADA itself defined a focal infection as; Sepsis arising from a focus of infection that initiates a secondary infection in a nearby or distant tissue or organs.
Mechanism of Focal Infection
Paraphrased from an article published in the Journal of the American Dental Association, Vol. 42, 1951
The concept of focal infection in relation to systemic disease is firmly established. The origin of many toxic or metastatic diseases may be traced to focus (a localized area), or focal areas of infection.
- Focus of infection: Focus of infection refers to a localized, circumscribed area infected with micro-organisms which may or may not give rise to clinical manifestations.
- Focal Infection: Whereas, focal infection refers to sepsis arising from a focus of infection (see above) that initiates a secondary infection in a nearby or distant tissue or organs.
- Two major mechanisms of focal infection.
-
- An actual metastasis of organisms from a focus.
- The spread of toxins or toxic products from a remote focus to other tissues by the blood stream.
- Once bacteria creating infection pass the abscess area of the tooth, they may:
-
- Multiply in the blood setting up an acute or chronic septicaemia.
- Be carried live to a suitable nidus where they infect the surrounding tissue.
- Produce a slow, progressive atrophy with replacement fibrosis in various organs of the body.
- Relationship to allergic and immune reactions.
- The bacteria at the focus may undergo autolysis or dissolution. Some of the products of this dissolution, diffusing into the blood or lymph, may sensitize various tissues of the body. ‘A later diffusion of these products on reaching the sensitized tissue may call forth an allergic reaction.’
Related Information
- Focus on Foci Cancer: A Second Opinion, Josef M. Issels, M.D.
- Dental Foci Can Undermine Health
Given all of the research condemning the harm root canal therapy causes (directly and indirectly) it is unclear why any dentist would continue to administer RCT in their practice.
- Dr. Robert Gammal, BDS, has compiled a comprehensive document with over 650 references of published, scientific literature regarding focal infection and disease. Dead Teeth Can Affect Your Health - Focal Infection
- Root Canal Toxicity Toxic Element Research Foundation (TERF)
- Root Canal Therapy (detailed explanation why RCT should be discontinued)
- Root Canal - Removal and Replacement (options for filling the gap)
- Zirconia Dental Implants - Analysis: Is "metal-free" devoid of metals? Christian Gross
- Surgical Removal (surgical tooth removal should be painless)
- Aetiology of root canal treatment failure: Why well-treated teeth can fail Department of Endodontics, School of Dentistry, Estácio de Sá University, Rio de Janeiro, RJ, Brazil
- Root Canal Removal Protocol - excerpt from the Root Canal CoverUp Exposed Dr. George Meinig
- In Vitro Enzymatic Inhibition Associated with Asymptomatic Root Canal Treated Teeth
Root Canal Related Infection - What You Can Do
Toothache pain is the unpleasant symptom of infection (abscess) in the nerve of the tooth. Pulpitis is inflammation of dental pulp tissue (nerve, blood vessels and connective tissue), and can cause the tooth to die. There are two types of pulpitis:
- 1. Reversible Pulpitis
- Pulpitis may be reversed when the cause of the pulpitis has been removed and the tooth is repaired. In an effort to keep the tooth vital (alive), various therapies may be used.
- 2. Irreversible Pulpitis
-
Irreversible damage has been caused to the tooth nerve(s). In this case the dentist will recommend root canal therapy (RCT). Endodontists promote RCT to restore function and relieve pain.
Tooth infection can spread through the opening at the end of the root (apex) into the bone surrounding the tooth. The ligament around the bone (periodontal ligament) and the bone itself have a massive blood supply, so bacteria and toxins can be transported throughout the body. Another very important passage of transport is directly along nerve fibres and back to the brain. Infected tissue inside the tooth is essentially dead. Dead tissue breaks down and becomes gangrenous, producing gaseous and liquid by products.
Conventional dentistry typically recommends root canal therapy to resolve pain. Unfortunately, it is impossible to remove all of the dead tissue, impossible to sterilize the tooth, and also impossible to fill the canal and seal it. Therefore the best that root therapy will do is temporarily relieve pain while leaving dead, infected and gangrenous tissue in your body. And although it is not often discussed, a tooth that has received root therapy may itself be the cause of an abscess later. When the RCT filling extends beyond the end of the tooth, it can cause liquefaction necrosis of the bone (dissolves the bone). A condition which looks and behaves just like an abscess.
A dead tooth should always be removed completely. It is usually easier to fill the gap than to deal with the systemic diseases caused by keeping such a tooth in your head. The best solution by far is to eat a good diet, reduce your stress levels and practice very good oral hygiene. Anything which reduces your immune function should be avoided and that includes mercury-amalgam fillings and fluoride, (either in the drinking water or applied directly to your teeth by the dentist). It is always better to prevent decay rather than deal with its consequences. Robert Gammmal, BDS
Both the endodontists who support root canal therapy, and those who oppose the therapy, agree on at least one thing; that infection is the primary health concern. Whether infection is at the site of the tooth (focused), or elsewhere in the body (focal), the best defense against infection is a robust immune function. Using hTMA to identify metabolic dysfunction and guide a corrective nutritional healing protocol is a safe and effective method for strengthening the immune response.
Back to TopDental Amalgams
- 1845: American Society of Dental Surgeons asked it's members to sign a mandatory pledge promising not to use mercury amalgam fillings, due to the serious harm caused by using them.
- 1856: American Society of Dental Surgeons, because of its stance against dental amalgam, is disbanded due to loss of membership. Some members reorganized in 1860 naming themselves the American Dental Association (ADA).
Mercury is not safe at any level. Over time, an amalgam filling will expand and crack the tooth leading ultimately to its death. Conventional dentistry usually recommends root canal therapy to treat a dead tooth. And root canals are best avoided if you value your health.
- Safe Removal of Amalgam Fillings Presentation by the International Academy of Oral Medicine and Toxicology (IAOMT) Technical Assistance Programme for dental professionals (TAP).
In large measure, those martyred by dementia are showing the results of toxicity from mercury, aluminium, lead, cadmium, arsenic and other heavy metals. Their neurons have been poisoned. They are turned into Alzheimer's victims directly through the efforts of dentists who blindly follow the party line of their trade union organization, the ADA. Dr. Casdorph, M.D., Toxic Metal Syndrome
A problem with amalgam removal is that the procedure releases significant amounts of mercury into the system, even when done carefully. To help prevent the accumulation of toxic mercury into body tissues, it is important to have enough of the protective minerals available in your cells, such as iron and selenium. Dental surgery also is a stressful process that places a high demand on the minerals needed for you to recover. hTMA can identify whether your system can manage the procedure adequately, or if you should fortify your ability to respond before undergoing amalgam removal.
CAUTION: Amalgam removal and replacement should only be done when the patient's stress response capacity can handle the physical trauma of the event and the unavoidable exposure from release of some amounts toxic mercury into the system. Adequate resilience requires healthy tissue mineral levels of iron, selenium and zinc. When present in the proper ratios, these minerals will protect against mercury exposure. In addition, proper removal protocol must be followed by a qualified, experienced (holistic) dentist.
- Please review: Safe Removal of Amalgam Fillings
Due to their high mercury content, so called "silver" dental amalgam fillings can endanger health. Amalgam emits mercury vapor even after it is implanted into the body. This mercury is bioaccumulative, and it crosses the placenta to accumulate in the fetus as well. Dental amalgam's mercury is a known health risk, especially for children, fetuses, nursing infants, and people with impaired kidney function.
- Chronic Mercury Poisoning: A Brief Summary of the Science
- Mercury Dental Amalgam: New Evidence Counters Old Notion that Amalgam is Safe Kristin G. Homme
- How mercury amalgam fillings destroy teeth
- World Mercury Project.org
Amalgam fillings are 50% mercury and release mercury vapor every time you chew, brush your teeth or drink something hot. Neither mercury based preservatives like thimerosal or amalgam have been subjected to proven safe by toxicological testing. The average person does not know that mercury is the second most toxic element on the planet, nor do they know that it is an incredibly potent toxin even at small exposure levels. Once in the body, mercury has a high affinity for moving into the brain where it can become trapped for decades. Once in the brain, mercury causes a chronic inflammatory process in the tissue which has been connected to autism, Alzheimer's, multiple sclerosis, amyotrophic lateral sclerosis (ALS or Lou Gehrig's disease) and many more adverse health consequences. Mercury at very low levels of exposure can induce symptoms identical to those of many devastating psychological, neurological and behavioral conditions in children and adults that currently have no known cause. Mercury is known to injure the senses, central nervous system, immune system, gastrointestinal system, kidneys, and to interfere with critical cellular pathways creating widespread havoc throughout the body. For more information:
Mercury and Fertility
In a 1993 study titled: ‘The effect of occupational exposure to mercury vapour on the fertility of female dental assistants,’ researchers found that mercury accumulates in the brain, pituitary, and thyroid, and that it disrupts ovulation in animals. They further state that women exposed to mercury experience abnormal menstrual cycles and suggest that mercury vapor may impair fertility in humans. The study demonstrated that the fecundability (probability of conception each menstrual cycle) of women who prepared 30 or more amalgams per week and who had five or more poor mercury hygiene factors, was only 63% of that for unexposed women (95% CI 42%-96%) after controlling for covariates.
A Small Dose of Toxicology provides an introduction to toxicology. Written by Dr. Steven G. Gilbert, director of The Institute of Neurotoxicology and Neurological Disorders (INND).
A Small Dose of Toxicology, published by The Institute of Neurotoxicology and Neurological Disorders explores the principles of toxicology by examining the health effects of common chemical agents. Information about the health effects of mercury can be found on page 108, in the chapter entitled A Small Dose of Mercury
The U.S. Food and Drug Administration (FDA) concedes that the developing neurological systems of children and fetuses are more susceptible to "the neurotoxic effects of mercury vapor," and that there is no evidence that amalgam is safe for these populations.
Water and wastewater/sewer authorities around the world have collectively identified dental offices as the major source of mercury pollution in wastewater. Amalgam is not chemically stable and does not break down in the environment. Regulatory action is in place in many jurisdictions requiring dental offices to install mercury wastewater separators. The health and environmental impacts of dental mercury are well understood 1-25. Mercury is considered a hazardous material before it is used, and a hazardous waste after it's removal, why not when it is put in your mouth as dental amalgam, slowly and continuously emitting mercury vapor?
Health Effects of Exposure to Mercury
Author: Steven G. Gilbert, PhD, DABT
- Inorganic Mercury
- Elemental mercury in the form of mercury vapor is readily and rapidly absorbed into the blood stream when inhaled and easily crosses the blood-brain barrier and the placenta. Oral ingestion of elemental mercury is far less hazardous than inhalation of mercury vapor due to its poor absorption in the gut. Acute, high level exposure to mercury vapor can result in respiratory, cardiovascular, neurological, and gastrointestinal effects, and even death. Both acute, high-dose exposure and chronic, low-dose exposure to mercury vapor can result in increasing and irreversible neurological effects. Symptoms include tremors and loss of feeling in the hands (paresthesia or stocking-glove sensory loss), emotional instability, insomnia, memory loss, and neuromuscular weakness. Exposure to mercury vapor may precipitate tremor, drowsiness, depression, and irritability; such symptoms form the basis for the expression "mad as a hatter" and the character the Mad Hatter in Lewis Carroll's Alice's Adventures in Wonderland. Decreased performance on memory tests and verbal concept formation have also been documented in industry workers exposed to mercury vapor. Neurotoxic effects such as dizziness, weakness, insomnia, numbness, and tremor were observed in a 12-year-old girl exposed to spilled mercury.
- Organic Mercury
-
The devastating health consequences of methyl mercury (MeHg) exposure were well documented from several tragic incidents. Historically, MeHg exposure played a very important role in drawing worldwide attention to the consequences of industrial pollution, not just for workers but also for the general public. In the 1950s, the consequences of MeHg exposure to the people of Minamata and Niigata, Japan were recognized. In both cases MeHg exposure resulted from consumption of fish from waters receiving industrial effluent discharge containing mercurials, which demonstrated conclusively that MeHg poisoning could occur through food-chain transfer of MeHg.
By 1974 over 2,150 cases of what was then called Minamata disease had been established in the Minamata region alone. Observations of an abnormally high incidence of cerebral palsy-like symptoms with involvement of the visual, sensory, and auditory systems among children from the Minamata region also heralded a new concern over the potential developmental toxicity of industrially derived MeHg. However, as with the adult cases of MeHg poisoning, establishing a causal relationship between environmental MeHg and cases of observed infantile developmental toxicity was difficult because the affected children had not eaten fish and there were no identified neurological effects in their mothers, based on evaluations at that time. The susceptibility and the sensitivity of the fetus to MeHg induced neurotoxicity were later documented in other studies.
A tragic incident in Iraq clearly documented the fetal effects of maternal methyl mercury exposure (see case study section). During the winter of 1971 some 73,000 tons of wheat and 22,000 tons of barley were imported into Iraq. This grain, intended for planting, was treated with various organic mercurials. Unfortunately, this grain was made into flour and consumed throughout the country, resulting in the hospitalization of some 6,530 people and the death of 459 at the time of the study. The accumulated evidence leaves no doubt that MeHg is a serious developmental toxicant in humans, especially to the nervous system. While the toxicological and behavioral outcomes resulting from high-concentration in utero exposures are not in debate, questions regarding risks and mechanisms of action following low concentration, chronic in utero exposures remain.
A US National Research Council report states that, "over 60,000 newborns annually might be at risk for adverse neurodevelopmental effects from in utero exposure to MeHg (methyl mercury)." This report clearly makes the point that many infants are exposed to mercury above levels considered safe.
One of the complications with diagnosing MeHg exposure is that presentation of symptoms appears to occur after a latency period during which no effects are observed. The period of latency appears to be related to the level of exposure, with higher exposure concentrations resulting in a shorter latency period. The exact biological mechanisms underlying this latency period are unclear. Some researchers have suggested that latency not only reflects the time to reach accumulation of MeHg in the brain, but also reflects achievement of a threshold wherein enough tissue is destroyed that the capacity of the CNS to compensate for the damage is overwhelmed. Observation of long latencies following cessation of MeHg administration in animals and humans, however, may also derive from long-term demethylation of MeHg to inorganic mercury in the brain.
Environmental Exposure to Mercury
EcoHealth magazine covers many of the issues presented and discussed at the Eighth International Conference on Mercury As a Global Pollutant conference. Papers include information on mercury toxicity and the mitigating role of selenium, how mercury moves through the ecosystem, and the global problem of low-level exposures.
The International Association for Ecology and Health sponsored Eighth International Conference on Mercury As a Global Pollutant held in Madison, Wisconsin, had over 1000 scientists from around the world. They came to share their understanding of the environmental fate of this pervasive contaminant.
"Few environmental health issues demand a transdisciplinary research agenda that spans such a wide range of disciplines—from biogeochemistry and ecosystem ecology to epidemiology and participatory action research—as environmental exposure to methylmercury (MeHg). Also, among the classic environmental health issues involving human and wildlife exposures to persistent and global contaminants (e.g., lead and organochlorides), MeHg remains the least resolved, in terms of both science and policy. The global nature of Hg is due to a number of factors: (1) It is generated largely from coal-fired power plants which are increasing worldwide; (2) it is atmospherically transported from these sources to eventual deposition on all land and water surfaces; and (3) it is transferred to humans through fish consumption which knows no international or socioeconomic boundaries." EcoHealth, Volume 5 Number 4Back to Top
Screening for Mercury Toxicity
Mercury poisoning can happen from an acute exposure but it is typically the consequence of chronic exposure. Hair tissue biopsy and urine challenge tests are types of screening recognized as valid for detecting chronic mercury toxicity. A urine test is performed after receiving a dose of a chelating agent. Urine or blood testing without a chelator will usually not reveal mercury toxicity unless the poisoning is acute. Alternative testing methods include electrodermal screening, muscle testing, and radionics. Kinesiology, electrodermal testing and radionics are subject to operator bias and other interference that can influence the test.
Toxins almost always come in synergistically acting package-deals. Mercury alone is toxic. Together with zinc it is many times more toxic, add in a little copper and silver, as in dental amalgam fillings, and the detrimental effect to the body increases manifold. Dr Dietrich Klinghardt PhD, physician and neurobiologist
No screening detection method is 100% accurate. Hair tissue biopsy results may not show high levels of mercury because it may be locked up in body tissues and is not being excreted in the hair. Urine challenge tests also may not show mercury that is sequestered deep inside body tissues. And biochemistry is complex, for example, mercury toxicity often accompanies copper toxicity.
hTMA does much more than detect mercury. hTMA, when properly performed and interpreted, assesses how the body is responding to stress. Test results can guide the correction of body chemistry to improve Adenosine-5'-triphosphate (ATP) production for intracellular energy transfer. ATP transports chemical energy within cells for metabolism. Enhanced metabolism facilitates the removal not only of mercury, but of cadmium, arsenic, lead, aluminum and many other toxic substances. Everyone has some level of mercury toxicity due to its wide distribution in the soil, our food, water, vaccines and dental materials. However, mercury may not be revealed on a first hair analysis unless it is being eliminated through the hair. Also, your individual metabolism, mineral levels and ratios will effect your ability to eliminate mercury. As this balance is improved, changes in mercury elimination will be seen on hTMA results.
Detoxification Methods
Five methods are effective for eliminating mercury toxicity and other toxic metals. Best results are realized when these methods are used in combination.
- hTMA. Improving cellular energy production enhances the body's natural ability to eliminate heavy metals.
- Antagonists. hTMA guided nutritional supplementation acts to counteract or replace toxic minerals (metals) by including bioavailable (preferred) minerals such as zinc and selenium.
- Chelators. Vitamin C, sulfur-containing amino acids and synthetic chelating drugs such as DMPS or DMSA. Nutritional methods to enhance metallothionein will also help the body chelate mercury.
- Excretion systems. Excretion is the process by which waste products of metabolism and other non-useful materials are eliminated from an organism. This is primarily carried out by the lungs, kidneys and skin. Mercury is eliminated primarily through the liver and kidneys. Supportive therapies can include supplements, physical therapy, NIR therapy, and enema therapy.
- Eliminate, reduce and mitigate exposure. Identify the sources of mercury and other toxic exposures. Take appropriate steps to resolve or minimize exposure risk.
Toxic metals are metals that form poisonous soluble compounds and have no biological role, i.e. are not essential minerals, or are in the wrong form. Using hTMA mineral balancing to resolve metal toxicity has an additional benefit in that it will avoid unbalancing the body chemistry. Using chelators as an example, both vitamin C and zinc are helpful for reducing mercury toxicity. However, excessive vitamin C or zinc will lower tissue copper levels. This will make some patients' condition worse. hTMA ensures a safe elimination process based on your biochemical individuality.
It is a common mistake to believe that mercury detoxification can be achieved in a short time frame (weeks or months). A variety of biological systems are affected by mercury toxicity. Also, most mercury toxicity is chronic, and continued exposure is probable. Therefore, although symptomatic improvement may occur rapidly, reducing mercury toxicity can take six months to several years. It is not unusual to see mercury elimination occurring several years after beginning the hTMA mineral balancing protocol. This can occur when the preferred minerals are not available in appropriate levels and ratios to protect against the use of mercury for tissue and enzyme building processes. Once healthy nutrient mineral levels are achieved, properly operating cellular detoxification functions can eliminate any mercury resulting from new exposures (rather than storing it).
Back to TopThe Surgeon General's Report on Oral Health
Oral health is integral to general health; this report provides important reminders that oral health means more than healthy teeth and that you cannot be healthy without oral health. The report outlines existing safe and effective disease prevention measures that everyone can adopt to improve oral health and prevent disease.
Back to Top
Resources
- Root Canal Therapt (RCT) Information
-
- Aetiology of RCT FailureSchool of Dentistry Dept. of Endodontics, Estácio de Sá University, Brazil
- Socket (ridge) Preservation Tooth extraction and jawbone preservation.
- Overview of Dental Pulp: Functions and Responses to Injury AU Dental Journal
- Dead Teeth Can Affect Your Health - Focal Infection (650+ root canal references)
- Root Canal Therapy (RCT) (detailed explanation why RCT should be discontinued)
- Root Canal Therapy Toxicity Toxic Element Research Foundation (TERF)
- Root Canal - Removal and Replacement (options for filling the gap)
- Zirconia Dental Implants - Analysis: Is "metal-free" devoid of metals? Christian Gross
- Surgical Removal (surgical tooth removal should be painless)
- Root Canal Removal Protocol excerpt from - Root Canal CoverUp Exposed by Dr. George Meinig
- In Vitro Enzymatic Inhibition Associated with Asymptomatic Root Canal Treated Teeth
- Say NO to Root Canals Leslie Kenton
- Avoid Root Canal
- Valplast® Flexible partial dentures, option for filling gap from removed tooth.
- Flexite Company Flexible partial dentures, option for filling gap from removed tooth.
- Root Canal Cover-up: Exposed
- Root Canal Cover-Up George A. Meinig DDS
- General Dental Health Information
-
-
The regeneration of tooth enamel, the hardest biological tissue, remains a considerable challenge because its complicated and well-aligned apatite structure has not been duplicated artificially. This report (download pdf above) shows a rationally designed material which mimics the biomineralization crystalline-amorphous frontier of hard tissue development in nature. After repair, the damaged enamel can be recovered completely because its hierarchical structure and mechanical properties are identical to those of natural enamel. The suggested phase transformation–based epitaxial growth follows a promising strategy for enamel regeneration.
Report: Repair of Tooth Enamel by Biomimetic Mineralization - Tooth-Organ Meridian Chart Prevention and Healing, Inc by Simon Yu, MD
- Nutrition and Physical Degeneration Weston A. Price (1939)
- Dental Infections - Oral and Systemic - Volume I Weston A. Price (1923) 500 pages
- Dental Infections - Oral and Systemic - Volume II Weston A. Price (1923) 700 pages
- Pathology of Dental Infections and Relation to General Diseases Weston A. Price (1916)
- The Ideal Oral Health Routine Guide to maintaining excellent oral fitness.
- Correct Toothbrushing Technique Scott Frey, DDS
- Are topical fluorides good for teeth? Short Answer: Yes.
- The 12 Best and Worst Foods for Your Teeth
- Making the Right Dental Choice By Bob Marshall, PhD, CCN
- Mercury Toxicology Hazards of mercury amalgam fillings.
- Oral Infections and Implications: S.H.Shakman with George Meinig
- Dental terminology List of commonly used terms of location and direction in dentistry.
- Most Wisdom Tooth Extraction Totally Unnecessary Sarah Pope
- Cure Tooth Decay Ramel Nagel
- Better Dentistry Information about dental treatments.
- Robert Gammal B.D.S. Information about various dental issues.
- Healing Teeth Naturally. healingteethnaturally.com
- Interactive Meridian Connection Tool
- Dental Ozone
- Tooth Chart Relationships between teeth and other areas of the body
- Jaws: Story of a Hidden Epidemic Sandra Kahn, Paul R. Ehrlich
-
The regeneration of tooth enamel, the hardest biological tissue, remains a considerable challenge because its complicated and well-aligned apatite structure has not been duplicated artificially. This report (download pdf above) shows a rationally designed material which mimics the biomineralization crystalline-amorphous frontier of hard tissue development in nature. After repair, the damaged enamel can be recovered completely because its hierarchical structure and mechanical properties are identical to those of natural enamel. The suggested phase transformation–based epitaxial growth follows a promising strategy for enamel regeneration.
- Biological Dentistry
-
The best dentistry is dentistry that avoids or eliminates harmful procedures and focuses on improving patient health. Biological dentistry is an example. When repair or intervention is required, minimal invasive techniques are used.
Back to Top
- Flouride Information
-
- Fluoride Dr. David Kennedy (DDS)
- Fluoride (short 51 second segment)
- Fluoride Action Network fluoridealert.org
- The Fluoride Deception Interview With Christopher Bryson
- New Study Links Water Fluoridation To Hypothyroidism
- Fluoridegate Documentary
- Fluorosis Fluorosis is a defect of tooth enamel caused by too much fluoride intake during the first 8 years of life. Although fluorosis can be cosmetically treated, the damage to the enamel is permanent. Common causes of fluorosis include: fluoridated drinking water (particularly during infancy), ingestion of fluoride toothpaste, use of fluoride tablets, and consumption of processed foods made with fluoridated water.
- The Case Against Fluoride by Paul Connett PhD
- Toxicity Information
-
- Scientific Case Against Amalgam International Academy of Oral Medicine and Toxicology, Stephen M. Koral, DMD
- Mercury Toxicology Toxicological profile for mercury (update) US Department of Health and Human Services
- Long-Term Effects of Chronic Low-Dose Mercury Exposure Walter - J. Crinnion, ND
- Mercury Exposure and Children's Health
Acute or chronic mercury exposure can cause adverse effects during any period of development. Mercury is a highly toxic element; there is no known safe level of exposure. Ideally, neither children nor adults should have any mercury in their bodies because it provides no physiological benefit. Prenatal and postnatal mercury exposures occur frequently in many different ways. Pediatricians, nurses, and other health care providers should understand the scope of mercury exposures and health problems among children and be prepared to handle mercury exposures in medical practice. Prevention is the key to reducing mercury poisoning. Mercury exists in different chemical forms: elemental (or metallic), inorganic, and organic (methylmercury and ethyl mercury). Mercury exposure can cause acute and chronic intoxication at low levels of exposure. Mercury is neuro-, nephro-, and immunotoxin. The development of the child in utero and early in life is at particular risk. Mercury is ubiquitous and persistent. Mercury is a global pollutant, bioaccumulating, mainly through the aquatic food chain, resulting in a serious health hazard for children. This article provides an extensive review of mercury exposure and children's health. - World Health Organization urges a switch in use of dental materials away from amalgam. The report includes the known toxic effects of mercury exposure. Future Use of Materials for Dental Restoration
- Smoking Teeth - Statement of concern regarding the amount of mercury leaking from silver amalgam fillings. Presentation transcript (photos and graphs)
- Smoking Teeth Presentation showing mercury vapor outgassing from a 25-year-old silver amalgam filling in an extracted tooth.
- The Dangers of Mainstream Dentistry Dr. Brian Clement explains the damaging effects of mainstream dentistry on your health. Find out about the dangers of mercury fillings, root canal filled teeth, the effect of dentistry on the energy meridians. Learn how to best take care of your teeth.
- The Many Dangers of Dental Metals Dr. Alison Adams
- Trace Amounts Official Trailer. Autism and vaccines.
- How mercury causes brain neuron damage. University of Calgary Faculty of Medicine Dept. of Physiology and Biophysics
- KJ's Story A 15 year-old poisoned by mercury fillings.
- Toxic Elements Research Foundation TERF is a non-profit research foundation dedicated to informing the public of potential problems associated with dental materials and procedures.
- Dental Amalgam Mercury Solutions (DAMS). DAMS will send you a free information package with contact information for recommended holistic dentists. They publish an informative newsletter you can subscribe to and help support their efforts. Amalgam.org
- Do you have Mercury Poisoning?
- The Coalition for Mercury-free Drugs (CoMeD)
- World Mercury Project
- ToxicTeeth is working to get mercury fillings outlawed. toxicteeth.org
- Dental sealants and composite fillings Dangerously high levels of bisphenol A (BPA)
- Dental X-rays double brain tumour risk
- Dental X-rays link to thyroid cancer
- U.S. Dept. of Health and Human Services Toxicological Profile for Mercury (Update)
- Dental Toxicity
- It's All in Your Head: The Link Between Mercury Amalgams and Illness Hal A. Huggins
- The Secret Poison in Your Mouth: Banish the Hidden Cause of Cancer, Heart Disease and Arthritis by M.L. Sarlin
References
- Masi, JV. Corrosion of Restorative Materials: The Problem and the Promise. Symposium: Status Quo and Perspectives of Amalgam and Other Dental Materials, April 29-May 1, (1994).
- Haley BE 2007. The relationship of the toxic effects of mercury to exacerbation of the medical condition classified as Alzheimer's disease. Medical Veritas, 4:1510–1524.
- Chew CL, Soh G, Lee AS, Yeoh TS. 1991. Long-term dissolution of mercury from a non-mercury-releasing amalgam. Clin Prev Dent, 13(3): 5-7.
- Gross, M.J., Harrison, J.A 1989. Some electrochemical features of the in vivo corrosion of dental amalgams. J. Appl. Electrochem., 19: 301-310.
- Richardson GM, R Wilson, D Allard, C Purtill, S Douma and J Gravière. 2011. Mercury exposure and risks from dental amalgam in the US population, post-2000. Science of the Total Environment, 409: 4257-4268.
- Hahn LJ, Kloiber R, Vimy MJ, Takahashi Y, Lorscheider FL. 1989. Dental "silver" tooth fillings: a source of mercury exposure revealed by whole-body image scan and tissue analysis. FASEB J, 3(14): 2641-6.
- Hahn LJ, Kloiber R, Leininger RW, Vimy MJ, Lorscheider FL. 1990. Whole-body imaging of the distribution of mercury released from dental fillings into monkey tissues. FASEB J, 4(14): 3256-60.
- USEPA (United States Environmental Protection Agency). 1995. Mercury, elemental (CASRN 7439-97-6). Integrated Risk Information System. Last updated June 1, 1995. www.epa.gov
- CalEPA (California Environmental Protection Agency). 2008. Mercury, Inorganic – Chronic Reference Exposure Level and Chronic Toxicity Summary. Office of Environmental Health Hazard Assessment, California EPA. Dated December 2008. Summary: www.oehha.ca.gov; Details: www.oehha.ca.gov
- Ngim, C-H., Foo, S.C., Boey, K.W. et al. 1992. Chronic neurobehavioral effects of elemental mercury in dentists. Br. J. Ind. Med., 49(11): 782-790.
- Richardson, GM, R Brecher, H Scobie, J Hamblen, K Phillips, J Samuelian and C Smith. 2009. Mercury vapour (Hg0): Continuing toxicological uncertainties, and establishing a Canadian reference exposure level. Regulatory Toxicology and Pharmacology, 53: 32-38.
- Lettmeier B, Boese-O'Reilly S, Drasch G. 2010. Proposal for a revised reference concentration (RfC) for mercury vapour in adults. Sci Total Environ, 408: 3530-3535.
- Fawer, R.F., de Ribaupeirre, Y., Buillemin, M.P. et al. 1983. Measurement of hand tremor induced by industrial exposure to metallic mercury. Br. J. Ind. Med., 40: 204-208.
- Piikivi, L., 1989a. Cardiovascular reflexes and low long-term exposure to mercury vapor. Int. Arch. Occup. Environ. Health 61, 391–395.
- Piikivi, L., Hanninen, H., 1989b. Subjective symptoms and psychological performance of chlorine-alkali workers. Scand. J. Work Environ. Health 15, 69–74.
- Piikivi, L., Tolonen, U., 1989c. EEG findings in chlor-alkali workers subjected to low long term exposure to mercury vapor. Br. J. Ind. Med. 46, 370–375.
- Suzuki, T., Shishido, S., Ishihara, N., 1976. Interaction of inorganic to organic mercury in their metabolism in the human body. Int. Arch. Occup. Environ.Health 38, 103–113.
- Echeverria, D., Woods, J.S., Heyer, N.J., Rohlman, D., Farin, F.M., Li, T., Garabedian, C.E., 2006. The association between a genetic polymorphism of coproporphyrinogen oxidase, dental mercury exposure and neurobehavioral response in humans. Neurotoxicol. Teratol. 28, 39–48.
- Mackert JR Jr. and Berglund A. 1997. Mercury exposure from dental amalgam fillings: absorbed dose and the potential for adverse health effects. Crit Rev Oral Biol Med 8(4):410-36.
- Richardson, G.M. 1995. Assessment of mercury exposure and risks from dental amalgam. Prepared on behalf of the Bureau of Medical Devices, Health Protection Branch, Health Canada. 109p. Dated August 18, 1995. dsp-psd.communication.gc.ca or publications.gc.ca
- Richardson, GM and M. Allan. 1996. A Monte Carlo Assessment of Mercury Exposure and Risks from Dental Amalgam. Human and Ecological Risk Assessment, 2(4):709-761.
- US FDA. 2009. Final Rule For Dental Amalgam. www.fda.gov
- Expanded from: Richardson, GM 2003. Inhalation of mercury-contaminated particulate matter by dentists: an overlooked occupational risk. Human and Ecological Risk Assessment, 9(6): 1519 – 1531. Figure provided by the author via personal communication.
- Roels, H., Abdeladim, S., Ceulemans, E. et al. 1987. Relationships between the concentrations of mercury in air and in blood or urine of workers exposed to mercury vapor. Ann. Occup. Hyg.,31(2): 135-145.
- Skare I, Engqvist A. Human exposure to mercury and silver released from dental amalgam restorations. Arch Environ Health 1994;49(5):384–94.