Update: 19 December 2024
Vitamin D
Author: David L. Watts, Ph.D., Director of Research Trace Elements, Inc.
We tested ultraviolet LEDs from different sources and at different wavelengths. RayVio's 293nm LED showed the most significant potential for vitamin D3 production in the shortest amount of time. This study will lead to a new generation of technology that can be labeled as photopharmacology in which the use of LEDs with targeted wavelengths can cause specific biologic effects in human skin to help treat and prevent chronic illnesses. Dr. Holick, Professor of Medicine, Physiology and Biophysics at Boston University School of Medicine, and endocrinologist at Boston Medical Center
Contents
- Nutritional, Hormonal, and Metabolic Effects of Vitamin D
- Assessing Individual Requirements for Vitamin D
- Vitamin D and Weight Loss?
- Vitamin D and Infections
- Anti-Bacterial Effects of Vitamin D and Anti-Viral Effects of Vitamin A
- Vitamin D and Cancer Prevention
- Cancer, Vitamin D and Metabolic Types
- Vitamin D and the Immune System
- Vitamin D Requirements
- Questions and Concerns about Vitamin D
- Resources
- References
What are the potential benefits, and pitfalls, of vitamin D therapy? According to some reports, vitamin D is good for weight loss, the prevention of several cancers, and it may help prevent influenza (among other claims). Some studies support increasing vitamin D intake, others do not.12
Nutritional, Hormonal, and Metabolic Effects of Vitamin D

Most everyone is aware of the functions of vitamin D in relation to the role it plays in building and maintaining the integrity of bones and teeth. From a mineral standpoint, vitamin D is most closely associated with the mineral calcium (Ca), affecting both its absorption and regulation. Rickets and osteomalacia are two major conditions related to vitamin D deficiency. Phosphorus (P) is also affected by vitamin D, as well as the balance between Ca and P in the body. The minerals zinc (Zn), copper (Cu), potassium (K), sodium (Na), magnesium (Mg) and others are also impacted by vitamin D status. Vitamin D also shares a synergistic and antagonistic relationship with other vitamins as well, which will be discussed later.
Vitamin D is actually a pro-hormone, the precursor to the production of calcitriol. Some of the major hormones that are related to, or affected by vitamin D include estrogen, progesterone, testosterone, insulin, thyroid, parathyroid and the adrenal hormones. Vitamin D can have a synergistic or promoting effect on some endocrine glands and their hormones and conversely, an inhibiting or antagonizing effect upon others.3 From a metabolic standpoint we consider vitamin D a parasympathetic, anabolic nutrient. Thus vitamin D has a sedative effect on metabolic activity in general. This is due to vitamin D's influence on certain vitamins and minerals as well as it's effect on the parasympathetic neuroendocrine and immune systems.4
Assessing Individual Requirements for Vitamin D
In order to assess a person's need for extra vitamin D we must view them as individuals rather than making broad assumptions based upon general population studies or disease processes. One must also be aware of individual metabolic types and the influence of vitamin D as well as any other nutrient, or substance that can effect that particular metabolic type. Those of you who are familiar with our metabolic typing though hTMA patterns will remember that we categorize individuals into eight metabolic types which fall under the two major categories, the Fast and Slow Metabolic types.
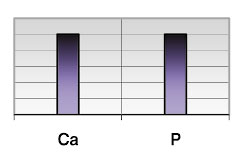
Figure 1. Normal calcium/phosphorus (Ca/P) ratio, indicating an ideal balance between the two minerals as well as adequacy of vitamin D.
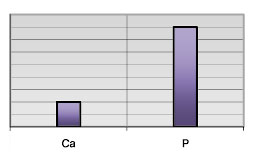
Figure 2. Low Ca/P ratio, indicating that vitamin D requirement is relatively increased for an individual with this tissue mineral pattern

Figure 3. Ca is dominating the picture relative to P therefore, vitamin D requirement would be much less for this particular mineral pattern.
Note: To emphasize the relationship of vitamin D to calcium and phosphorus, additional nutrient minerals, which also are influenced by vitamin D, are not shown in these diagrams.
Approximately seventy-five percent of the American population is found to be in the Slow Metabolic category and the other twenty-five percent are in the Fast Metabolic category. Knowing a person's metabolic type alone provides a greater understanding of a person's need for vitamin D, thus providing optimum clinical benefit and more importantly avoiding the potential adverse effects of too much vitamin D.
The vitamin D issue really presents us with a dilemma. I think vitamin D supplementation looms as the next big health disaster after vaccines, psychotropic drugs, statin drugs, antibiotics, GMOs, and calcium supplementation. Dr. Rick Malter
As mentioned previously vitamin D not only affects the absorption of the minerals calcium (Ca) and phosphorus (P), it also helps in regulating the normal balance between the two. The ideal hTMA Ca level is 60 milligrams percent (mg%) with a range of 22 to 97 mg%. The ideal P level is 16 mg% with a range of 11 to 20 mg%. However, the relationship between these two minerals is far more important than maintaining their respective normal levels or ranges. The ideal balance or ratio between Ca and P is 2.63 to 1 with a range of 1.6 to 3.6. From this relationship alone we can approximate the need for vitamin D for an individual. Figure 1 shows a normal Ca/P ratio, indicating an ideal balance between the two minerals as well as adequacy of vitamin D. Figure 2 is showing a low Ca/P ratio, indicating that vitamin D requirement is relatively increased for an individual with this tissue mineral pattern. In the next illustration (Figure 3) we can see that Ca is dominating the picture relative to P therefore, vitamin D requirement would be much less for this particular mineral pattern.
Vitamin D via its effect upon Ca also affects the minerals magnesium (Mg) sodium (Na) and potassium (K). The next illustration (Figure 4) shows the ideal balance between Ca/Mg, Ca/K and Ca/Na. When the Ca/ K and Ca/Na ratio is low (Figure 5) then vitamin D requirements are increased. A reverse of these ratios would indicate a reduced need for vitamin D. The ideal relationship between Ca and Mg can also be disrupted by vitamin D status. An elevated Ca/Mg ratio in the slow metabolic type would indicate that vitamin D needs are reduced and that vitamin D therapy should be reduced in a patient with this mineral pattern.
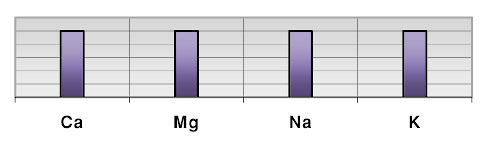
Figure 4. Ideal balance between Ca/Mg, Ca/K and Ca/Na.
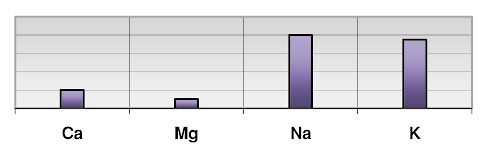
Figure 5. When the Ca/ K and Ca/Na ratio is low then vitamin D requirements are increased.
The minerals zinc (Zn) and copper (Cu) can also provide an indication of vitamin D requirements. An elevated Zn/Cu ratio may indicate an increased requirement, while a low Zn/Cu ratio may indicate a reduced need for vitamin D depending upon the metabolic type.
Vitamin D and Weight Loss?
Recently there has been a great deal of buzz in the popular press claiming a significant role for the increased intake of vitamin D, calcium and dairy for weight loss. At present the evidence of increasing dairy, calcium and vitamin D for aiding weight loss is inconclusive. This is due to the fact that the groups involved in the study also consumed a low calorie weight loss type of diet.
From hTMA studies weight loss will not occur simply by increasing the dietary intake of calcium, vitamin D and milk for most people, but may be beneficial for some. Since approximately seventy-five percent of the U.S. population fall into the slow metabolic category and since vitamin D as well as calcium are sedative, increasing their intake would further sedate the slow metabolic type. This is due to several factors. Probably the number one factor is that excess vitamin D and calcium will reduce thyroid and adrenal expression.5 Calcium absorption is actually increased in the presence of low thyroid activity. This can be attributed to increased parathyroid hormone activity which increases with under-activity of the thyroid. Low thyroid activity in turn leads to reduced adrenal activity. Therefore, increased intake of vitamin D, calcium and dairy can further reduce the metabolic rate in a person who is already predisposed, resulting in a reduction of caloric expenditure and weight gain instead of desired weight loss. Further, vitamin D shares a synergistic relationship to insulin and parathyroid hormone (PTH).
Insulin, also an anabolic hormone as well as having lipogenic properties, enhances the synthesis of vitamin D and conversely vitamin D enhances the synthesis of insulin. Both of which influence the production of PTH, another anabolic hormone, all of which can further reduce metabolic activity through suppression of the thyroid with a corresponding decrease in adrenal activity. The cumulative effects result in a reduced metabolic rate and a corresponding reduction in the burning of calories. The combined effects of vitamin D, calcium, PTH and insulin along with increased intake of dairy products would more likely contribute to further peripheral (hips and thighs) fat deposition and weight gain rather than weight loss in the majority of the population of slow metabolic types.
On the other hand, fast metabolic groups, approximately 25 percent of the population, may benefit from increasing dairy products, vitamin D and calcium resulting in weight loss instead of weight gain, specifically in those with abdominal obesity.6 Fast metabolic types are more prone to the metabolic syndrome and have the tendency for abdominal or central fat deposition which is influenced by the opposite endocrine involvement than that of the slow metabolic population. That is, an increased metabolic rate contributed to by increased thyroid and adrenal cortical activity with low PTH activity and insulin antagonism. Vitamin D, calcium and dairy would have a reducing effect on the over-activity of the thyroid and adrenal hormones, enhance PTH activity which in turn would enhance calcium absorption and increase the action of insulin.
Vitamin D and Infections
Many people have asserted that the seasonal increase in the incident of the flu virus may be due to vitamin D deficiency. This is a logical assumption since vitamin production from irradiation of the skin by the sun is less in winter months. Studies have shown that supplementing cod liver oil reduces the incidence of viral infections in children during the winter months.7 However, at TEI we classify vitamin D as having a more anti-bacterial activity than anti-viral.8 We have classified vitamin A as being anti-viral.9 There is little research in this area, but what does exists supports our anti-bacterial and anti-viral classifications of vitamins D and A.
The studies that showed a reduction in viral respiratory infection in children during winter months used a cod liver oil supplement. It is true that cod liver oil is a source of vitamin D; however it contains over ten times more vitamin A than vitamin D. Perhaps the anti-viral effect attributed to vitamin D was erroneous in these studies owing to the markedly increased intake of vitamin A in these children from the cod liver oil supplements.
Anti-Bacterial Effects of Vitamin D and Anti-Viral Effects of Vitamin A
Numerous studies have shown the effectiveness of vitamin D against bacterial infections. 10 11 12 Specifically, vitamin D has been used in the treatment of tuberculosis during the pre-antibiotic era. Photo therapy was also successful for the treatment of lupus vulgaris or tuberculosis of the skin since sun exposure naturally increased vitamin D production.13 Our classification of the anti-bacterial effects of vitamin D as well as its pro-viral effects is based upon vitamin D's relationship with Ca, P, Cu Zn and Fe. An increase in the tissue concentration of Ca is known to enhance the activity and proliferation of dormant viruses whereas, increasing tissue concentrations of P inhibits viral activity.14 Increased tissue calcium accumulation is of course enhanced by vitamin D. Low tissue Cu is associated with increased susceptibility to bacterial infections.15 Vitamin D is synergistic to the mineral Cu. Since the Fe/Cu ratio or balance is also important for the prevention of Cu deficiency induced bacterial infections, both vitamin D and Ca are antagonistic to Fe. Lastly, vitamin D has been found to enhance the production of HIV.16/ Our hTMA studies have shown individuals with ARC and AIDS have a slow metabolic mineral pattern in conjunction with a markedly low Zn/Cu ratio.17 Vitamin A is well known to combat viruses. The papilloma virus is suppressed by vitamin A and it has been found that HIV-1 replication is inhibited by vitamin A. 18 19 Seroconversion to measles vaccine and inhibition of the herpes simplex virus replication has been noted with vitamin A therapy.20 21 Animal studies have shown the antiviral effects of vitamin A on the canine distemper virus as well.22 Vitamin A is synergistic to Zn a mineral known for its antiviral effects. Vitamin A also reduces tissue Ca concentrations relative to P.
Vitamin D and Cancer Prevention
The potential role of vitamin D in protecting individuals from developing cancer has gained a great deal of interest over the past year. Some evidence is supportive while some is negative and yet others reveal no association. 23 24 Light can be shed on this dilemma when cancer is viewed from a metabolic standpoint via tissue mineral analysis studies and the interrelationship between vitamin D and other nutrients, endocrine and immunological factors.
Cancer, Vitamin D and Metabolic Types
Often malignancies are classified as being hormonally sensitive or hormonally driven. However, cancer development is most often contributed to by a myriad of factors and not merely a single entity such as an individual hormone, vitamin deficiency, bacteria, virus or xenobiotic. It would be best to view malignancies as being caused by a number of multiple, complex interrelated factors including the environment, neurological, endocrine, metabolic, immunological and nutritional status. We typically see specific hTMA patterns and metabolic categories associated with various types of malignancies which can therefore be categorized into Sympathetic or Parasympathetic conditions. This allows the recognition of the specific coexisting factors involving malignant conditions including the neuroendocrine-immunological-metabolicnutritional-environmental factors.
Incidence of Malignant Breast Tumors and Metabolic Types as Recognized From hTMA Studies
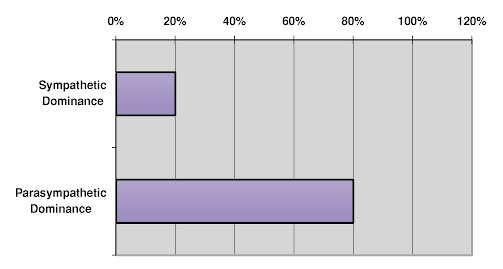
Figure 6. Slow metabolic mineral pattern, or ‘parasympathetic dominance.’
For instance, so called estrogen driven tumors are most often seen in individuals who are showing a slow metabolic mineral pattern or Parasympathetic Dominance. (See Figure 6) Therefore, an elevated tissue Ca and Cu are common along with an elevated Ca/Mg, Ca/P and low Zn/Cu. A malignancy in this pattern could be considered as being driven by the Parasympathetic neuroendocrine-immune-nutritionalmetabolic systems. This metabolic pattern does indicate estrogen dominance, but other factors are involved as well including insulin, PTH, and cellular immune dominance.25 26 In this case involving elevated tissue calcium, vitamin D may only be acting in concert with Ca to encase a malignant growth such as a breast tumor in an effort to prevent metastasis. The serum level of vitamin D has been found to be elevated in individuals with early stage breast cancer.27
Whether this is causative or a result of the malignancy remains to be determined. However, we can speculate that in such a case, vitamin D would not be preventive, but may very well be acting as a protective agent against metastasis. Since some malignancies are known to be related to underlying viral initiators with corresponding over-active cellular immune activation, vitamin D therapy would not be related to prevention. However, from our previous discussions we can strongly speculate that vitamin A would be preventive.
Incidence of Prostate Cancer and Metabolic Types as Recognized From hTMA Studies
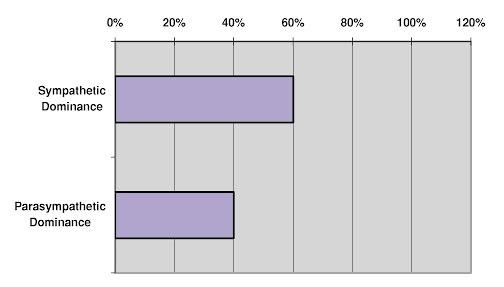
Figure 7. Tissue mineral patterns of low Ca and Cu, low Ca/P with elevated Fe/Cu and Zn/Cu ratios.
Malignancies that are not so-called estrogen-driven, but may be called androgen or progesterone driven (See Figure 7) is most often seen in tissue mineral patterns of low Ca and Cu, low Ca/P with elevated Fe/Cu and Zn/Cu ratios. This pattern could be termed a Sympathetic condition involving the sympathetic neuroendocrineimmune-nutritional-metabolic systems with adrenal cortical, thyroid, testosterone and humoral immune dominance, with low insulin, estrogen and PTH. A deficiency of copper as well as an excess of Fe leads to increased production of free radicals resulting in significant cellular damage. In this instance vitamin D and its synergistic cofactors may well be preventive. On the other hand we can surmise that increased vitamin A intake would further enhance the Sympathetic malignancy.
Cancer Incidence in Adult U.S. Population and Metabolic Types as Recognized From hTMA Studies
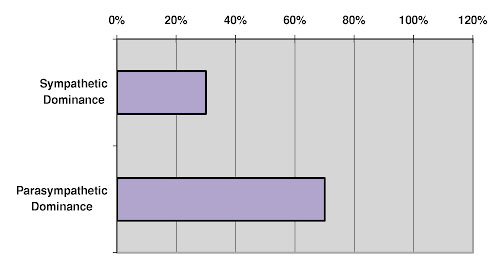
Figure 8.
The scenarios discussed above can also help determine where vitamin A fits into this picture. Since vitamin A has the opposite effects of vitamin D, vitamin A may be helpful in preventing malignancies that could develop in patients with a slow metabolic rate.
Vitamin D and the Immune System
Both vitamins D and A are synergistically involved in the normal immune response. In certain circumstances, vitamin A and D are also antagonistic to each other. We consider vitamin D having a more pronounced effect on the cellular immune response. Too much vitamin D could precipitate a cellular auto-immune response in susceptible individuals. Whereas, vitamin A is closely related to the humoral immune response and excessive intake could lead to a dominant humoral autoimmune response.
Vitamin D Requirements
Based upon some of the above cited studies and from test results of blood levels of vitamin D, it is being suggested that the recommended daily allowance (RDA) for vitamin D be raised. Some propose up to 1000 I.U. per day for the general adult population. This may be an unwise step until further investigations are completed. The action of vitamin D does not depend upon adequate serum levels alone. Although circulating levels of vitamin D are related to dietary intake and synthesis from solar radiation, its conversion to an active form may be lacking in some individuals.
Vitamin D receptors, other enzymes, hormones and nutritional status and nutritional interrelationships all affect vitamin D requirements. We have discussed the relationship of vitamin D to Ca, Mg, P, Zn, Cu, Fe, vitamin A, the hormones insulin, estrogen, progesterone, androgen, PTH, the immune system as well as the thyroid and adrenal activity adding up to over a dozen factors that are known to affect vitamin D status. Actually there are numerous other relationships, far too many to be discussed within the confines of this cursory review. Suffice it to say that tissue mineral analysis can reveal many of these significant interrelationships and can be an intricate tool in assessing individual vitamin D requirements.
Questions and Concerns about Vitamin D
There is almost not a day that goes by that I am not asked questions about vitamin D, even though our reports state if vitamin D supplementation is necessary or not for that particular individual. Patient's who show a low blood vitamin D level think they should take extra vitamin D even though they fall into a slow metabolic pattern. This is certainly not the case by any means. In fact, there seems to be a movement to make vitamin D the magic bullet that cures just about everything. Even the normal blood ranges for vitamin D have been proposed to be arbitrarily raised with no substantive evidence for doing so.
In some circles it has been suggested to double and even quadruple the normal level of vitamin D from the present ranges with little regard for individual metabolic circumstances. Since these artificially raised "normal" levels are extremely difficult to attain, many practitioners and organizations are now recommending mega dosages of vitamin D with seemingly little regard for the long-term risks and complications this can cause.
Recently the Institute of Medicine (IOM) released a statement suggesting that raising the normal range for vitamin D as well as suggesting long-term high intake of vitamin D is not warranted at this time. Further their report stated that after reviewing hundreds of studies and reports of the beneficial effect of vitamin D playing a protective role against cancer, heart disease, diabetes and autoimmune disease, the studies are conflicting and provide mixed results. Apparently, there is not enough evidence to confirm that vitamin D has these effects. Other studies confirm this report by the IOM. An assessment of data from the Third National Health and Nutritional Examination Survey (NHANES III) came to similar conclusions, and also discussed the adverse effects of high blood vitamin D levels on mortality rates. Apparently, cancer mortality did not correlate with serum vitamin D levels in a total population studied. However, in some the higher vitamin D levels were related to a higher cancer mortality rate compared to those with lower vitamin D levels. Freedman, Dm et al. Serum 25hydroxyvitamin D and cancer mortality in the NHANES III study. Cancer Res. Nov.1, 2010.
These conflicting reports and studies can be explained based upon hair tissue mineral analysis (hTMA) studies. The proper recommendations for vitamin D intake and supplementation can also be better applied and explained through hTMA studies.
- Slow Metabolism:
-
We have found that the higher the tissue levels of calcium, the less stored vitamin D will be converted to the active form. In the Slow Metabolic Type, the tissue level of calcium is elevated, which is contributed by a relative dominance of the parathyroid. This can be termed primary hyperparathyroidism or subclinical hyperparathyroidism. This type of hyperparathyroidism resulting in excess tissue calcium concentrations reduces the formation of active vitamin D. This is why oftentimes Slow Metabolic Types will show low normal active vitamin D levels. Unfortunately, raising active vitamin D in the blood to higher levels is difficult, even with mega dosing of vitamin D through supplements. However, when the subclinical hyperparathyroidism is brought under control, the blood level of active vitamin D will increase, even without vitamin D supplementation. Forcing an increase in blood vitamin D levels with pharmacological amounts of vitamin D is similar to forcing the reduction of cholesterol levels with medications and expecting it to prevent cardiovascular disease. As we can see from the previous discussion, this does little good and may actually cause harm in the long-term.
For example, Vitamin D can further exacerbate parathyroid expression, contributing to cellular autoimmune conditions, soft tissue calcifications, renal stone formation, osteoarthritis, osteoporosis and CVD. In some cases, a deficiency of vitamin D can cause secondary hyperparathyroidism leading to rickets and osteomalacia, conditions that respond readily to vitamin D supplementation. This condition is rare compared to the incidence of primary hyperparathyroidism. For more information on the impact of hyperparathyroidism and vitamin D you might want to visit the following website of the Norman Parathyroid Center at Tampa General Hospital, https://www.parathyroid.com. This website provides extensive information related to parathyroid disorders as well as their view regarding vitamin D levels. Their information actually supports the findings I have discussed previously based upon our hTMA test results.
- Fast Metabolism:
On the other hand, the Fast Metabolic Type does in fact have low hTMA calcium levels and also an increased need for vitamin D. However, this group makes up only about twenty-five percent of the population in comparison to Slow Metabolic Types.
Vitamin D therapy in the Fast Metabolic Group will have beneficial effects of reducing or preventing certain types of cancers, heart disease, as well as reducing excessive humoral autoimmune conditions.
- Download: Vitamin D
Future research should seek to clarify if and for whom there may be an increased risk for cancer at particular sites with high 25 (OH)D concentrations, and the concentrations at which this risk increases. The health status, life stage, adiposity, estrogen exposure and nutritional status of study participants should be taken into account. Continued investigation is necessary to ensure that vitamin D recommendations are appropriately targeted to individuals who stand to benefit most, while protecting vulnerable subgroups from risk of overexposure. The Vitamin D and Cancer Conundrum: Aiming at a moving target.
Resources
- LED lights safer, more effective in producing Vitamin D3 than sunlight Boston Univ School of Medicine
- Research Challenges Vitamin D Deficiency
- Largest Clinical Study on Vitamin D: We're Wrong About One of Its Main Benefits
- The Science behind vitamin D - Autoimmunity Research Foundation
References
- Vitamin D – Gives Strong Bones, Weight Loss, Too? www.weightcontrolroom.com. Dec. 2007.
- Preventing vitamin D deficiency – The new breakthrough? www.womentowomen.com. Dec. 2007.
- Mineral Imbalance, Endocrines and Hair Tissue Mineral Analysis. Watts, DL. TEI Newslett. 6,2, 1993.
- Trace Elements and Other Essential Nutrients. Watts, DL. Writers BLOCK. 1997.
- Weight Control Through Metabolic Control. Watts, DL. TEI Newslett. 4,4,1990.
- Metabolic syndrome X – As Defined Through hTMA Patterns. Watts, D.L. TEI Newslett. 17. 1,2. 2007.
- Epidem. and Infection. 134,6. 2006.
- Calcium and Virus Activation. Watts, DL. TEI Newslett. 3,5.1989.
- The Nutritional Relationships of Vitamin A. Watts, DL. J. Orthomol.Med. 6,1. 1991.
- Tuberculosis and Vitamin D Deficiency. Sasidharan, PK, et al. J. Assoc. Phys. India. 50, 2002.
- Vitamin D in the Treatment of Pulmonary Tuberculosis. Martineau, AR, et al. J. Steroid. Biochem. Mol.Biol. 103, 2007.
- A Single Dose of Vitamin D Enhances Immunity to Mycobacteria. Martineau, AR, et.al. Am.J.Respir.Crit.Care Med. 176,2. 2007.
- Finsen NR (1886). Om anvendelse i medicinen af koncentrerede kemiske lysstraaler. Copenhagen, Denmark: Gyldendalske Boghandels Forlag.
- Calcium and Virus Activation. Watts, DL. TEI Newslett. 3,5.1989.
- The Nutritional Relationships of Copper. Watts, DL. J.Orthomol,Med. 4,2. 1989.
- Effect of 1,25-dihydroxyvitamin D3 and its Analogs on Human Immunodeficiency Infection in Monocytes/Macrophages. Kizaki, M, et.al. Leukemia. 7,10. 1993.
- The Immune System and Hair tissue Mineral Patterns. Nutritional, Neuro-endocrine Immunology. Watts, DL. TEI Newslett. 7,1. 1994.
- Retinoic Acid Suppresses Human Papillomavirus Type 16 (HPV16)-Mediated Transformation of Human Keratinocytes and Inhibits the Expression of the HPV16 Oncogenes. Creek, KE, et.al. Adv.Exp.Med.Biol. 354. 1994.
- All-trans Retinoic Acid Attacks Reverse Transcriptase Resulting in Inhibition of HIV-1 Replication. Maeda, Y, et.al. Hematol. 12,3. 2007.
- Inhibition of Herpes Simplex Virus Replication By Retinoic Acid. Isaacs, CS, et.al. Antivral. Res. 33,2.1997.
- Enhancement in Seroconversion to Measles Vaccine with Simultaneous Administration of Vitamin A in 9-Month-Old Indian Infants. Bhaskaram, P, et.al. Ind. J. Ped. 64,4. 1997.
- Disease Manifestations of Canine Distemper Virus Infection in Ferrets are Modulated by Vitamin A Status. J.Nutr. 137,8. 2007.
- Vitamin D and Cancer: Current Dilemmas and Future Needs. Davis, CD, et.el. Nutr.Rev. 65,8. 2007.
- Epidemiological Studies of Vitamin D and Breast Cancer. Rohan, T. Nutr. Rev. 65,8. 2007.
- Insulin, Insulin-Like growth Factors, Insulin resistance and Neoplasia. Pollak, MN. Am.J.Clin.Nutr. 86,3. 2007.
- Increased Prevalence of Primary Hyperparathyroidism in Treated Breast Cancer. Fierabracci, P, et.al. J. endocrinol. Invest. 24,5. 2001.
- Serum 25-hydroxyvitamin D Levels in Early and Advanced Breast Cancer. Palmieri, C., et.al. J. Clin.Pathol. 59,12. 2006.
Source: https://www.traceelements.com/ - Copyright ©2008 Trace Elements, Inc. All Rights Reserved.
Find a hTMA Practitioner Back to TopEditor's note: This article may or may not contain minor editing from the original document. Editing is done for one or more reasons: technical issues, layout or space considerations, content accuracy and/or clarity. © Copyrighted content is owned by the author. Please contact the author if you have any questions or would like to use any of their content for any reason whatsoever. Thank you.